
Following the United States Supreme Court ruling in Dobbs v Jackson on June 24, 2022, access to abortion has become much more restricted in parts of the country. As of January 2023, 12 states have effectively banned abortion with very limited exceptions and several more states have severely restricted abortion access.1 More bans and restrictions may follow. Although some pregnant people in states where abortion is banned or restricted may travel to receive care in states where abortion continues to be accessible, the current legal landscape makes it more likely that others will look for ways to induce an abortion without the direct guidance of a healthcare provider.
Evidence shows that even prior to the Dobbs v Jackson decision, 7% of people in the US attempt self-managed abortion (SMA) at some point in their lifetime.2 People may choose to self-manage an abortion due to restrictive abortion laws, cost, timeliness, or the convenience provided by avoiding transportation, travel, or the need to arrange childcare.3-5 It also may be seen as a way of preserving privacy or avoiding contact with the medical establishment where they may have experienced stigmatization or discrimination while receiving care.3,4 The new circumstances of abortion access in the US are likely to increase the incidence of SMA.6 Self-managed abortion is any action taken by someone to end a pregnancy outside of the traditional healthcare system. Self-managed medication abortion (SMMA) most commonly entails a person self-sourcing mifepristone and misoprostol, the same medications prescribed to manage miscarriage or for medication abortion. It is distinguished from obtaining the same medications through a clinical or telehealth visit with a healthcare provider.3
The purpose of this article is to provide nurse practitioners (NPs) with guidance when they encounter patients who seek their care before, during, or after an SMMA. Understanding patients needs and being able to recognize any complications may help prevent unnecessary morbidity and mortality related to SMMA.
Self-managed medication abortion options
Many people undergoing an SMMA will access misoprostol with or without mifepristone through an online source. Because misoprostol also is used to treat gastric ulcers, they may be able to obtain misoprostol by prescription for other means or from pharmacies outside the country without prescription.3,7
Data on medication abortion show it is safe and effective whether provided in a clinical setting, with a clinician via telehealth, and with or without the use of ultrasound dating.8,9 Serious complications requiring hospitalization, surgery, or blood transfusion are rare, occurring in less than 0.4% of cases.8,9 For pregnancies shorter than 11 weeks gestation, a combination of mifepristone and misoprostol is 91% to more than 99% effective at terminating a pregnancy depending on gestational age and dosing regimen.10 Misoprostol alone is a reasonable option when mifepristone is unavailable. A meta-analysis on the use of misoprostol alone for abortion in the first trimester estimated that it is 93% effective at terminating a pregnancy and results in transfusion or hospitalization in 0.2% of people.11 Evidence indicates that people can use these medications safely and effectively for the purposes of an SMMA.3,12
Despite its safety and effectiveness, people who undergo an SMMA may experience concerns or have questions about the process. The pregnant person must determine for themselves whether they are a candidate for SMMA, administer the medication, monitor the process, and self-assess whether the abortion is complete.12 For these reasons, they may seek information, advice, reassurance, or care from clinicians before, during, or after their SMMA.3
Legal considerations and SMMA
As an NP, the ability to provide recommendations, advice, or aspects of abortion care will depend on the laws in the state where the NP is practicing. NPs can consult with legal counsel about their medical-legal rights to assist patients in different scenarios before, during, or after SMMA. Several legal advocacy organizations offer assistance to clinicians providing abortion care as well as people who have had abortions in need of legal help (Table 1).
Because of the likelihood of encountering a patient who is planning, has attempted, or has completed an SMMA, NPs and other clinicians should consider how they will respond to these patients and what services they can provide while safeguarding themselves, their employer, and their patients from legal risk. For NPs working in states where abortion is illegal or severely restricted, general information can be provided in lieu of specific medical advice.13 Providing a patient who is considering SMMA with resources where they can obtain accurate information promotes safety for patients while avoiding providing direct medical advice and risk for legal action (Table 1).14

Some people may be wary of seeking care from a clinician/healthcare agency during or after an SMMA, even when they are experiencing signs or symptoms of potential complications. Their concern is not without merit. Three states have laws explicitly criminalizing SMA, and 24 have laws that could be used to do so.3,15,16 Despite this, there are currently no known laws that require healthcare providers to report a planned, attempted, or completed SMA to law enforcement.3,16 In fact, reporting protected health information (PHI) to law enforcement may violate not only the patients trust but also the patients right to privacy, which could result in civil and criminal penalties. The US Department of Health and Human Services released guidance in June 2022 concerning HIPAA compliance regarding abortion.17 The guidance advises healthcare providers that disclosing PHI to law enforcement is a HIPAA breach unless state law expressly requires reporting, and currently no state law has mandated reporting patients in this way.18
The state in which an NP is practicing will determine what level of involvement in abortion care they can provide. In states where abortion itself is not restricted, there may still be laws prohibiting clinicians who are not physicians from providing abortion care.19 In states where abortion is not restricted, NPs are able to provide guidance, medical advice, and services to the extent of their training and scope of practice.
Before SMMA
Nurse practitioners encountering patients considering SMMA should share information on any abortion restrictions in their state. One resource they can direct patients to is the Repro Legal Helpline to help them understand potential legal risks (Table 1).
The NP should assure that the patient is aware of all their pregnancy options: abortion with medication or a procedure, continuing the pregnancy and parenting, or placing the child for adoption. The NP also should assess for reproductive coercion. If the patient has chosen abortion, a discussion on seeking care from a telehealth or physical clinic as an alternative to SMMA is appropriate. Nurse practitioners who do not provide abortion information in their practice must be able to provide the patient with a prompt referral to someone who can provide this information in a timely manner.
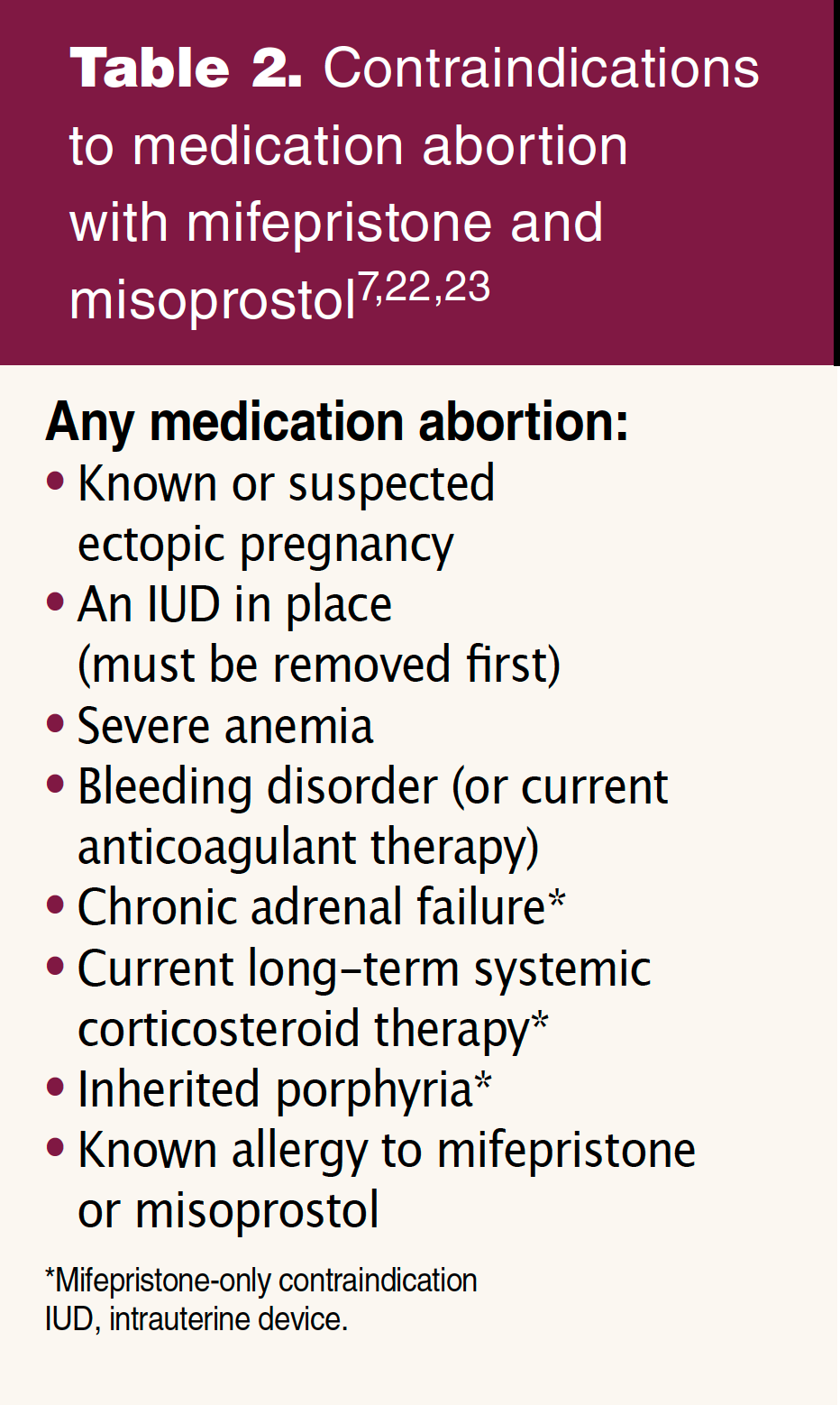 NPs also can help the person determine whether they are a candidate for or have contraindications to medication abortion by reviewing medical history and medications (Table 2). Some patients may need help calculating their estimated gestational age (EGA) based on their last menstrual period (LMP). These patients could be directed to an online gestational age calculator, or the NP could calculate it for them.3,13 Although people can typically estimate their EGA with accuracy based on LMP alone, some may seek care for an ultrasound to confirm their gestational age.3 People with signs or symptoms of ectopic pregnancy need sonographic evaluation.
NPs also can help the person determine whether they are a candidate for or have contraindications to medication abortion by reviewing medical history and medications (Table 2). Some patients may need help calculating their estimated gestational age (EGA) based on their last menstrual period (LMP). These patients could be directed to an online gestational age calculator, or the NP could calculate it for them.3,13 Although people can typically estimate their EGA with accuracy based on LMP alone, some may seek care for an ultrasound to confirm their gestational age.3 People with signs or symptoms of ectopic pregnancy need sonographic evaluation.
Patients can be made aware that abortion using mifepristone and misoprostol is safe and effective, and depending on legal limitations, NPs may be able to provide a list of where they can obtain reliable information on safely obtaining and using these medications (Table 1).3,13 Providing this information may prevent the patient from engaging in unsafe, toxic, or dangerous methods of SMA.3
During SMMA
Patients may have obtained the medication but need instructions on its use. Again, depending on the legal restrictions in the state where an NP is practicing, the NP may be able to provide guidance or direct the patient to a source known to provide evidence-based, easy-to-understand instructions (Table 1).
Some patients may have questions during the abortion about what to expect or what constitutes a cause for concern. If an NP is unable to provide advice personally, the Miscarriage and Abortion Hotline is a confidential, private, and secure hotline staffed by licensed clinicians 7 days a week who can provide support and information (Table 1).20
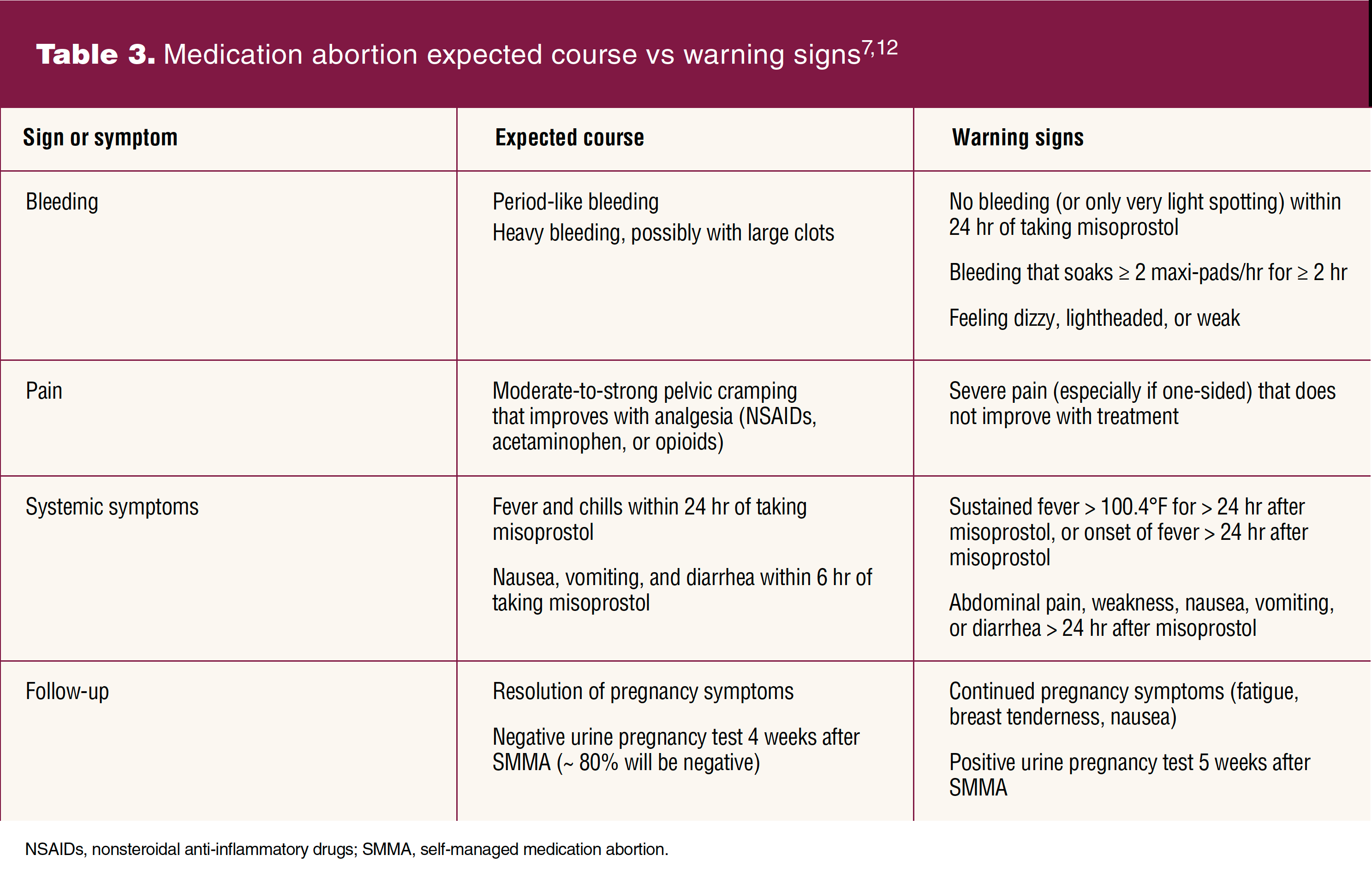
Most people who use mifepristone and misoprostol for SMMA will follow a typical course. Expected bleeding and cramping can be managed with reassurance and symptomatic treatment.3 It is important that NPs familiarize themselves with expected symptoms and their timing after a patient takes mifepristone and misoprostol so warning signs of potential complications can be identified (Table 3). As well, they can then determine who needs to seek urgent or emergent care. For people who present with concerns or complications, the differential diagnoses will center on ruling out acute conditions such as ectopic pregnancy, hemorrhage, sepsis, trauma, or exposure to toxins.16 Patients for whom there is concern about any of these should be evaluated in an emergency department.
Some people may be reluctant to seek care in an emergency department during or after an SMMA over concern they will encounter poor treatment due to clinician beliefs or bias, or that they will be reported to law enforcement. Patients can simply tell emergency department healthcare providers that they are pregnant and what they are experiencing — most often pain and/or bleeding.13 There is no blood test that will detect mifepristone or misoprostol levels.13 Clinicians in the emergency department will not be able to clinically distinguish an SMMA with mifepristone and misoprostol from a spontaneous abortion, and they do not need to do so.13,16 Their assessment should focus on a patients symptoms, not on differentiating the etiology of the pregnancy termination.3,16
After SMMA
People may seek care wondering if their abortion is complete. People who experience the expected bleeding and have resolution of pregnancy symptoms can typically be reassured that their abortion is complete. If a patient desires further confirmation, options include ultrasound, serial β-hCG measurement, or they can take a urine pregnancy test at home. Pregnancy tests can remain positive for several weeks following a complete abortion, so it is recommended to wait at least 4 weeks before taking one.3,21
People also may seek help for emotional support during or after an abortion. They can be directed to several confidential, nonjudgmental talk lines (Table 1).
Keeping people safe
Despite the changing legal landscape of abortion in the US, people will continue to seek abortions. Medication abortion is well established as a safe and effective option for many people with unwanted pregnancies, although it may carry legal risks to patients in some states. If an NP is uncertain about the abortion laws in their state, the Guttmacher Institute keeps up-to-date information available.19 Additionally, they could reach out to the Abortion Defense Network or their personal legal counsel for further information (Table 1).
Providing patients who are planning, undergoing, or who have completed an SMMA with accurate information in an unbiased and nonjudgmental manner may help destigmatize SMMA and abortion in general.12 Destigmatization may make patients more likely to seek care before, during, or after an SMMA if they need it. In situations where NPs are legally prohibited from providing abortion-related care, steering patients toward reliable sources of information can help those who choose SMMA to do so safely and decrease unnecessary morbidity and mortality.
Laurie L. Ray is Assistant Clinical Professor at Emory University Nell Hodgson Woodruff School of Nursing in Atlanta, Georgia. The author has no actual or potential conflicts of interest in relation to the contents of this article.
Editors note: The legal status of providing or obtaining mifepristone for medication abortion was in flux at the time this article went to press. Readers should remain cognizant of and follow current federal and state laws on the provision of mifepristone. BK
Womens Healthcare. 2023;11(3):26-31. doi: 10.51256/WHC062326
References
1 Nash E, Guarnieri I. Six months post-Roe, 24 US states have banned abortion or are likely to do so: a roundup. Guttmacher Institute. February 8, 2023. https://www.guttmacher.org/2023/01/six-months-post-roe-24-us-states-have-banned- abortion-or-are-likely-do-so-roundup.
2 Ralph L, Foster DG, Raifman S, et al. Prevalence of self-managed abortion among women of reproductive age in the United States. JAMA Netw Open. 2020;3(12):e2029245.
3 Verma N, Goyal V, Grossman D, et al. Society of Family Planning interim clinical recommendations: self-managed abortion. SFP Interim Clinical Recommendations. Updated September 8, 2022. https://doi.org/10.46621/ZRDX9581.
4 Aiken ARA, Starling JE, Gomperts R. Factors associated with use of an online telemedicine service to access self- managed medical abortion in the US.JAMA Netw Open. 2021;4(5):e2111852.
5 Aiken ARA, Broussard K, Johnson DM, Padron E. Motivations and experiences of people seeking medication abortion online in the United States.Perspect Sex Reprod Health. 2018;50(4):157-163.
6 Aiken ARA, Starling JE, Scott JG, Gomperts R. Association of Texas Senate Bill 8 with requests for self-managed medication abortion.JAMA Netw Open.2022;5(2):e221122.
7 Fleming M, Shih G, Goodman S; TEACH Collaborative Working Group. TEACH Abortion Training Curriculum, 7th ed. San Francisco, CA: UCSF Bixby Center for Global Reproductive Health; 2022. Bixby Doc: 2022-001(07/22).
8 Grossman D, Grindlay K. Safety of medical abortion provided through telemedicine compared with in person. Obstet Gynecol. 2017;130(4):778-782.
9 Aiken ARA, Lohr PA, Lord J, et al. Effectiveness, safety, and acceptability of no-test medical abortion (termination of pregnancy) provided via telemedicine: a national cohort study. BJOG. 2021;128(9):1464-1474.
10 National Abortion Federation. Clinical Policy Guidelines for Abortion Care. Washington, DC: National Abortion Federation; 2022. https://prochoice.org/providers/quality-standards/.
11 Raymond EG, Harrison MS, Weaver MA. Efficacy of misoprostol alone for first-trimester medical abortion: a systematic review.Obstet Gynecol. 2019;133(1):137-147.
12 World Health Organization. Abortion Care Guideline. Geneva, Switzerland: World Health Organization; 2022. https://www.who.int/publications/i/item/9789240039483.
13 Reproductive Health Access Project. Approach to Patients Undergoing Self-Managed Medication Abortion. September 27, 2022. https://www.reproductiveaccess.org/resource/approach-to-patients-undergoing-self-managed-medication-abortion/.
14 DAmbrosio A. Murky legal landscape for docs advising patients on self-managed abortions. MedPage Today. July 22, 2022. https://www.medpagetoday.com/special-reports/features/99867.
15 Huss L, Diaz-Tello F, Samari G. Self-Care, Criminalized: August 2022 Preliminary Findings. If/When/How. 2022. https://www.ifwhenhow.org/resources/self-care-criminalized-preliminary-findings/.
16 Harris LH, Grossman D. Complications of unsafe and self- managed abortion.N Engl J Med. 2020;382(11):1029-1040.
17 U.S. Department of Health & Human Services, Office for Civil Rights. HIPAA Privacy Rule and Disclosures of Information Relating to Reproductive Health Care. Updated June 29, 2022. https://www.hhs.gov/hipaa/for-professionals/privacy/guidance/phi-reproductive-health/index.html.
18 Watson K, Paul M, Yanow S, Baruch J. Supporting, not reportingemergency department ethics in a post-Roe era. N Engl J Med. 2022;387(10):861-863.
19 Guttmacher Institute. An Overview of Abortion Laws. Updated March 1, 2023. https://www.guttmacher.org/state-policy/explore/overview-abortion-laws
20 Miscarriage and Abortion Hotline. The Miscarriage and Abortion Hotline. 2022. www.mahotline.org.
21 Raymond EG, Anger HA, Chong E, et al. False positive urine pregnancy test results after successful medication abortion.Contraception. 2021;103(6):400-403.
22 Ipas. How to Have an Abortion with Pills. Chapel Hill, NC: Ipas; 2021. https://www.ipas.org/wp-content/uploads/2022/03/How-to-have-an-abortion-with-pills_ASCTW2E22.pdf.
23 American College of Obstetricians and Gynecologists Committee on Practice BulletinsGynecology, Society of Family Planning. ACOG Practice Bulletin no. 225. Medication abortion up to 70 days of gestation: Obstet Gynecol. 2020;136(4):e31-e47.
Web resources
A abortiondefensenetwork.org/
C reproductiverights.org/maps/abortion-laws-by-state/
I ipas.org/our-work/self-managed-abortion/abortion-with-pills/
J doctorswithoutborders.org/latest/how-ensure-safe-abortion-pills
K reproductiveaccess.org/abortion/sma/
P prochoice.org/providers/quality-standards/
Key words: self-managed abortion, self-sourced medication abortion, self-managed medication abortion