
Case study: The use of 3 patient scenarios to present, review and apply the latest advances in contraception as well as review a few contraceptive methods in development.
Awareness of the latest contraceptive advances could increase their use and increase patient options.
Introduction and Case Study:
F.G. is a women’s health practitioner with a busy office schedule today, including three patients that want to discuss contraception options.
- Patient 1, S. P., is a young college student that presents for a contraceptive appointment. She comes from a family where contraception is a sensitive topic and not openly discussed and she is unaware of different contraceptive options. S.P. currently takes traditional oral contraceptives but admits that she occasionally misses a dose here or there. S.P. says she is looking for an affordable method that works, has some flexibility, and doesn’t require a daily reminder. Her present lifestyle includes irregular sleep, stress and social activities. She has no significant medical history and is currently covered by her parents’ health insurance.
- Patient 2, R.G., is an attorney with a well-disciplined and structured lifestyle. R.G. is diagnosed with ADHD, and while she has previously struggled with anxiety and depression in the week leading up to her period, she has developed management methods that work well for her. R.G. wants to find a non-hormonal contraceptive method that will not introduce any new hormonal fluctuations. She has no further significant medical history and has the financial means to consider contraceptive options that are more expensive but offer convenience and effectiveness without hormonal side effects.
- Patient 3, M.K., is a single parent of two healthy children. She works full time and is unable to get time off from work often. She is looking for a contraceptive method that is compatible with her controlled hypertension. She takes time off to attend primary care appointments, so she is looking for a reliable method that does not require many office visits. Her reproductive health plan includes no future pregnancies, but she is not interested in a permanent option quite yet.
As noted in our case study above, women who seek reproductive control lead diverse lives, whether through their cultural background, economic status, or medical histories. Patient compliance and satisfaction have the potential to increase when diverse needs are acknowledged. Healthcare providers can provide further options to women by providing them with up-to-date information as they make their contraceptive choice. Below we have highlighted recent developments in contraceptive methods and explore some promising developments to better prepare providers to meet their patients’ diverse needs.
Anatomy and Physiology:
As provider F.G. considers the best options for her patients, she may begin by looking to the two broadest categories for contraception methods: hormonal and nonhormonal. Hormonal contraception uses either estrogen and/or progesterone to prevent pregnancy. Common examples include oral contraceptive pills, progesterone intrauterine devices or implants. Hormonal contraception prevents pregnancy through a three-pronged approach. First, hormonal contraception suppresses ovulation by inhibiting the release of Follicle Stimulating Hormone and Luteinizing Hormone.1 Next, it disrupts the proliferative and secretory phases of the endometrium, which thins the endometriallining and inhibits implantation.1 Lastly, hormonal contraception increases the viscosity of the cervical mucus affecting sperm mobility.1 The combination of these effects makes hormonal contraception highly effective, and therefore a popular patient choice in preventing unintended pregnancies.
By contrast, nonhormonal contraception does not alter a woman’s hormonal system. Rather, nonhormonal contraception functions by blocking or impairing sperm from reaching the egg, whether through physical or chemical means.2 Common examples include condoms, diaphragms or spermicide. While nonhormonal contraception methods do not boast the same efficacy as hormonal contraception methods, they may present fewer challenges for patients that otherwise struggle with ease of availability, hormone balance, or significant medical histories.
Contraception Methods: What’s New?
Over the counter progesterone only oral contraceptive pill (POP)
In March 2024, the U.S. Food and Drug Administration (“FDA”) approved its first over the counter (“OTC”) oralcontraceptive pill.3 It is a progestin (norgestrel) only, 28-day pill regimen that contains progestin.3
Practice Implications:
- OTC availability decreases the office appointment barrier for patients.
- Patients should take the pill daily within a 3-hour scheduled time. If they are late taking the pill, counsel the patient on use of back up methods for 48 hours with missed or late pills.3
- Side effects include irregular bleeding, headaches, dizziness, nausea, increased appetite, abdominal pain, cramps or bloating.3
- 99% effective with perfect use.6
- Approximate cost is $20 a month and is available online.4
Nonhormonal Contraceptive Gel
Patient controlled nonhormonal contraceptive vaginal gel contains lactic acid, citric acid, and potassium bitartrate. One prefilled applicator placed into the vagina before vaginal sex helps to maintain an acidic vaginal pH and reduces sperm motility.5
Practice Implications:
- Available by prescription5
- Administer immediately before or up to 1 hour before each act of vaginal intercourse 5
- Reapplication is necessary with more than 1 act of vaginal intercourse or occurrence > 1 hour after application5
- Use after vaginal sex reduces its effectiveness. The mechanism primarily works by prevention of sperm mobility. If inserted after sex, it won’t have the opportunity to block sperm before reaching the cervix.3,5
- Does not contain nonoxynol-9 which may reduce the risk of vaginal irritation, lowers risk of STI susceptibility, and is gentler on vaginal flora. 2
- May be used with other barrier and hormonal methods 5
- Potential microbicide for urogenital infection prevention5
- 93% effective with perfect use.5
- Cost is approximately $400/12 applications. However, may be covered by most insurance.6
Self-Administered Injectables
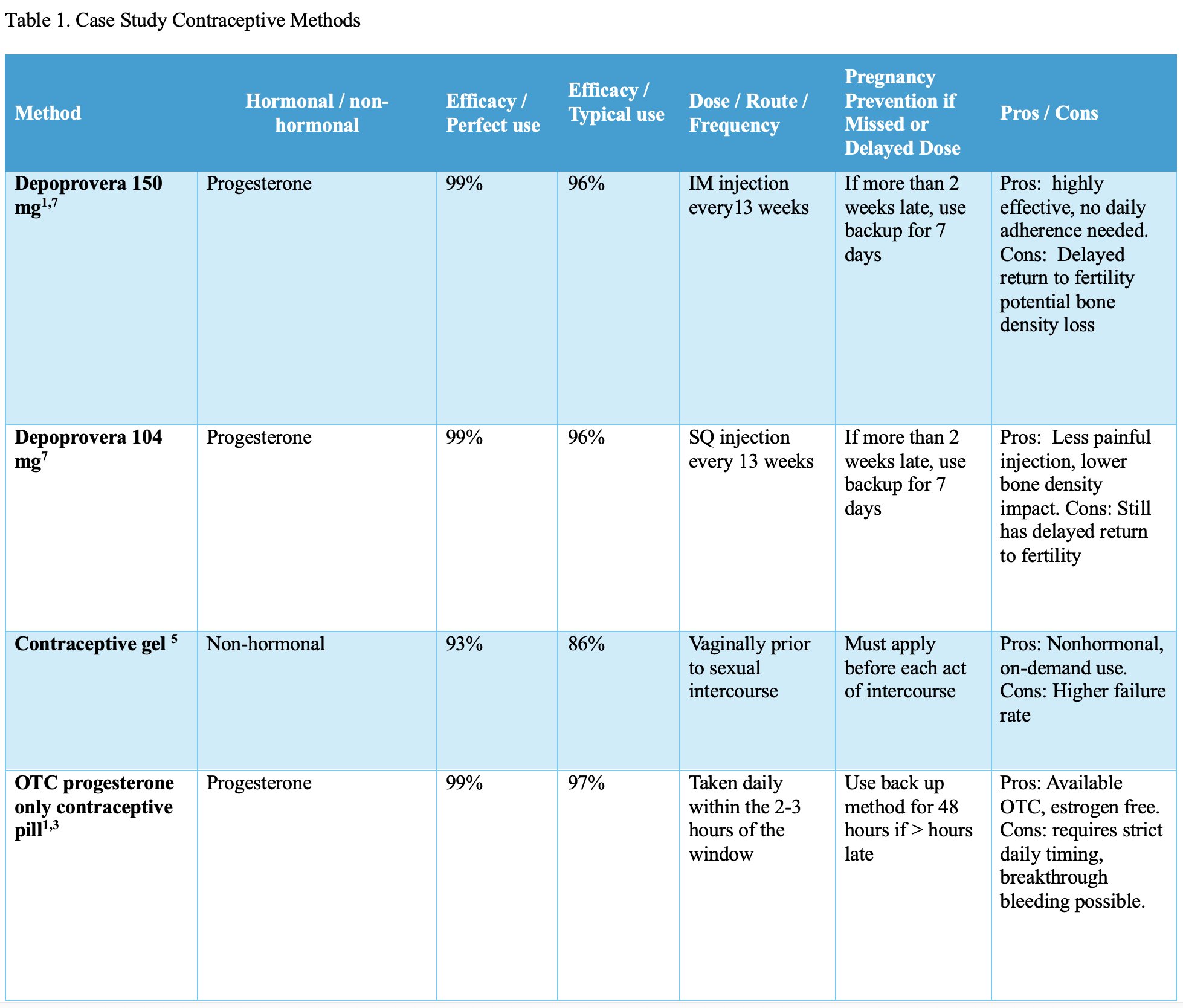
Depot medroxyprogesterone acetate (DMPA) is an injectable contraceptive method approved in in the United Statessince 2004. DMPA, can be administered subcutaneously or intramuscularly every 13 weeks.7 The differences between the two methods are listed in Table 1. DMPA has not been fully adopted for self-administration by the FDA, but was supported by the Center for Disease Control and Prevention and the World Health Organization in 2024.7 Self-administration offers patient control, shared decision making with increased access. Research studies support its feasibility and safety.7
Practice Implications:
- DPMA Subcutaneious (SQ) is approved by the FDA to be administered by a healthcare professional. Self-administered use is considered off label use.8
- Higher rates of continuation were observed with self-administration compared with provider administration.7
- DPMA IM 150 mg may be given every 13 weeks. If up to 2 weeks late no additional contraception is necessary.7
- DPMA SQ 104 , requires a backup method of contraception is needed after 13 weeks.7
- With initial implementation:
- Consider in person or Telehealth 8
- Review sharps disposal 8
- Review billing and reimbursement with administration 8
- Cost for 3 months is approximately $150 and may be covered by most insurance 9
Contraception Methods in Development
Biodegradable Implant
Contraceptive Implants are a long acting, reversible form of contraception. They release etonogestrel for up to a three-year period. The traditional implant requires appointments for both insertion and removal. In development is the biodegradable long term contraceptive implant.10 The biodegradable implant is the same as the traditional implant as it releases a slow amount of progestin. However, with the biodegradable properties, the implant would not require removal, therefore, decreasing the amount of office appointments and procedures required.10 Clinical trials are presently in phase II.10 Their present findings suggest that the implant is a safe and effective long-acting contraceptive.10 These findings need further confirmation in Phase III clinical trials with larger sample sizes.10
Practice Implications:
Practitioners should be aware that biodegradable implants are presently in research and development. This method will offer long term contraception for patients interested who have difficulty keeping office appointments or have anxiety with the removal procedure.
New Generation IUDs
The Copper Intrauterine Device is a nonhormonal contraceptive method approved by the FDA in 1984 and available since 1988 in the United States.11 It is a small, T shaped device that is placed in the uterus during an office procedure. It releases a small amount of copper which is spermicidal and is 99% effective in the prevention of pregnancy.11 In 2024, research is investigating lower copper amounts and changing the IUD to a more flexible and spherical or frameless shape.11 The new designs and dosages intend to ease insertion, reduce perforation, malposition and expulsion rates and decrease dysmenorrhea and menorrhagia.11
Practice Implications:
- Practitioners should be aware that the new generation Copper IUDs are being utilized and researched outside the United States. These new IUDs will offer easier insertion, less perforation risk and fewer side effects.
Conclusion:
Potential solutions for provider F.G. evaluating the three patients listed above using the latest advances in contraceptive options could include:
- Patient 1: DMPA SQ could be ordered for S.P. This contraceptive option would not require daily reminders and would minimize office appointments. This will allow the patient to attend college while using an effective form of contraception. The practitioner should confirm if the patient is willing to administer the SQ injections herself and whether it is covered by her insurance.
- Patient 2: Contraceptive gel would align well with the needs of R.G.. Contraceptive gels do not affect hormones and would not interfere with anxiety, depression or ADHD that G finds concerning. The practitioner could prescribe this medication giving the patient another nonhormonal option.
- Patient 3: K. could be offered the OTC POP pill for contraception. If prescribed and counseled on how to take correctly, this method would not require M.K. to attend office appointments and miss work. The POP would be compatible with her history of controlled hypertension. OTC POP pills may not be covered by insurance and does require the patient to take it consistently at the same time of day. The provider would need to review these limitations with M.K. Other alternative options may need to be explored after further discussions.
Advances in contraception allow women to tailor contraceptive options to their lifestyle. As women’s health practitioners, we are challenged to keep up to date with present and future methods giving women safe, effective and convenient options.
Monica Ketchie DNP, CNM, ANP, FACNM, is Associate Professor of Nurse Midwifery and Women’s Health Nurse Practitioner Coordinator at the School of Nursing, Georgia College & State University.
References
- Britton, E., Alspaugh, A., Greene, M. Z., & McLemore, M. R. (2020). CE: An evidence- based update on contraception. AJN, American Journal of Nursing, 120(2), 22-33. doi: https://doi.org/10.1097/01.naj.0000654304.29632.a7
- Howard SA, Benhabbour SR. Non-Hormonal Contraception. Journal of Clinical Medicine. 2023;12(14):4791. doi: https://doi.org/10.3390/jcm12144791
- S. Food and Drug Administration. FDA approves first nonprescription daily oral contraceptive. FDA; 2023. Accessed October 4, 2024. Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-nonprescription-daily-oral-contraceptivenonprescription-daily-oral-contraceptive
- How much does Opill cost? (n.d.). Drugs.com. https://www.drugs.com/medical-answers/how-opill-cost-3576594
- Baker, C. C., & Chen, M. J. (2022). New contraception update — Annovera, Phexxi, Slynd, and Twirla. Current Obstetrics and Gynecology Reports, 11(1), 21- 27. https://doi.org/10.1007/s13669-021-00321-4
- Phexxi Prices, Coupons, Copay & Patient Assistance. (n.d.). Drugs.com. https://www.drugs.com/price-guide/phexxi
- Curtis KM, Nguyen AT, Tepper NK, et al. (2024) U.S. Selected Practice Recommendations for Contraceptive Use. MMWR Recommendations and Reports;73(No. RR-3):1–77. DOI: http://dx.doi.org/10.15585/mmwr.rr7303a1
- A Toolkit for Self-Administration of Subcutaneous Depot Medroxyprogesterone Acetate A TOOLKIT FOR SELF-ADMINISTRATION OF SUBCUTANEOUS DEPOT MEDROXYPROGESTERONE ACETATE. (n.d.). Retrieved October 4, 2024, from https://ctcsrh.org/wp-content/uploads/User_Administration_DMPA-SC_Toolkit-002.pdf
- Depo-subQ provera 104 Prices, Coupons, Copay Cards & Patient Assistance. (n.d.). Drugs.com. https://www.drugs.com/price-guide/depo-subq-provera-104
- Yan, M., Zhang, Y., Wu, Z., Li, Y., Dou, K., Wang, B., Wang, Y., & Zhou, Q. (2022). Recent progress in advanced biomaterials for long-acting reversible contraception. Journal of Nanobiotechnology, 20(1). https://doi.org/10.1186/s12951-022-01329-5
- Bunting, J. J., Leung, Z. C., Boboc, B., Betts, D. H., Gilroy, J. B., Oinonen, K., Choi, K., Chambers, L., Rafea, B.A., & Gateman, S. M. (2024). Revolutionizing women’s health: The quest for materials for next-generation, non-hormonal intrauterine devices. npj Women’s Health, 2(1). https://doi.org/10.1038/s44294-024-00026-y