
Fibroids are benign uterine tumors that are the leading cause of hysterectomy in the United States. They may be asymptomatic or cause heavy menstrual bleeding, dysmenorrhea, bulk symptoms, and infertility. Multiple options exist for the treatment of fibroids and include expectant management, medical therapy, or surgical interventions. Nurse practitioners are an important part of the healthcare team and can assist women in making individualized decisions about treatment options based on their symptoms and reproductive life plans.
Key words: uterine fibroids, heavy menstrual bleeding, treatment, hysterectomy
Uterine fibroids, also called uterine leiomyomas or myomas, are benign uterine tumors that grow during the reproductive years and tend to regress after menopause.1 Fibroids can be asymptomatic and cause no adverse effects or can result in a range of symptoms for which woman may seek treatment. They are the leading reason for hysterectomy in the United States.1,2 Incidence and prevalence data can vary widely because asymptomatic women may not be aware they have fibroids and never receive a formal diagnosis. It has been estimated, however, that more than 75% of women may have at least one fibroid by the time they reach age 50 years.2 This estimate exceeds 80% among women of African descent.3 Considering the prevalence of fibroids, this article provides information on the diagnosis and management of fibroids and discusses treatment options for women who want to preserve their fertility.
The management and treatment of fibroids places an economic burden on both individual women and the healthcare system in the United States.4,5 Women with fibroids can incur direct costs associated with treatment, such as those associated with medications, surgery, and hospitalization, as well as indirect costs that include lost days of work, utilization of sick time, paid time off and short-term disability, and lost wages from uncompensated absences from work.4 Costs to the US healthcare system are estimated to be over 30 billion dollars per year.6
Epidemiology
Fibroids are monoclonal tumors that originate from the smooth muscle (myometrium) of the uterus and consist of extracellular matrix containing collagen, fibronectin, and proteoglycan.7 Cells within fibroid tumors are receptive to both estrogen and progesterone, and these receptors stimulate growth that happens during the reproductive years. Declining rates of estrogen and progesterone after menopause contribute to the regression of fibroids that occurs after the menopause transition.2 Fibroids are benign but can resemble leiomyosarcoma, a rare form of uterine cancer. Endometrial biopsy and magnetic resonance imaging (MRI) may help determine if sarcoma exists, but a definitive diagnosis can only be made through biopsy of the fibroid tissue.3
Risk factors
Certain factors have been associated with an increased risk of developing fibroids. Women of African descent have the highest risk of fibroids compared with women of all other racial or ethnic backgrounds.8 Age is also an important factor. Women who are age 40 to 50 years are more likely to have fibroids than younger women.9 Other factors such as an early menarche (< age 10 years), a family history of fibroids, obesity, and nulliparity have also been associated with the development of fibroids.9 Women who smoke, are multiparous, had a later menarche (> age 16 years), and have used oral contraceptives are less likely to develop fibroids.2
Symptoms
For many women, fibroids are asymptomatic. Women who have symptoms may present with heavy menstrual bleeding (HMB) and dysmenorrhea. The heavy bleeding may lead to a clinically significant anemia. Other women complain of bulk symptoms from an enlarged uterus, which could include pelvic pressure, back pain, bloating, urinary frequency, and dyspareunia.10 Women who are seeking pregnancy may experience infertility, subfertility, and recurrent pregnancy loss.10 Because symptoms have a gradual onset and could be explained by a variety of benign conditions, women often delay seeking a diagnosis by 3 to 4 years.6,11
Diagnosis
Transvaginal ultrasound is the most common imaging modality for the diagnosis of fibroids. A bimanual pelvic exam may reveal an enlarged or irregularly shaped, nontender uterus and palpable firm masses, but diagnosis is confirmed by ultrasound, which helps determine where the fibroids are located.11 Intramural fibroids are the most common and grow within the wall of the uterus. Subserosal fibroids grow on the outside of the uterus and can put pressure on surrounding organs if they become large. Submucosal fibroids grow just below the uterine lining and can extend into the uterine cavity, distorting the size and shape of the cavity. Pedunculated fibroids are less common and grow on a stalk outside of the uterus.11 Although not a first-line imaging modality due to cost, MRI can be helpful in providing more detail about fibroid location and size, especially if there are multiple large fibroids, body habitus limits ultrasonography results, fibroids extend outside of the uterine cavity, transvaginal ultrasound is not tolerated, or if surgery is being considered.10,11
HMB with the finding of an enlarged uterus or mass is clinically suggestive of fibroids but can also be caused by other conditions. Adenomyosis, which is growth of endometrial glands and stroma within the myometrium, can cause heavy bleeding. On exam, the uterus is often enlarged, globular in shape, and tender.2 Masses may be caused by endometriosis and carcinoma of the uterus and ovaries. Uterine polyps and endometrial hyperplasia can also result in HMB.3 Although rare, uterine sarcoma, which closely resembles benign fibroids on ultrasound, is possible. Pathologic evaluation of any mass is the only way to definitively differentiate between benign and malignant tumors.2,3
Impairment of fertility
Fibroids have the ability to impair fertility, but size, number, and location are important factors. Submucosal fibroids may cause anatomic changes that distort the size and shape of the uterine cavity. This can alter the endometrium, interfere with endometrial blood supply, and potentially affect implantation and increase the risk of spontaneous pregnancy loss. Fibroids can also increase uterine contractility and are associated with preterm delivery, lower birthweight infants, breech presentation, and surgical birth.4,12
Treatment
Depending on a woman’s symptoms, number of fibroids, and location, there are multiple treatment options. Additionally, a woman’s age and whether she wishes to preserve her fertility are important aspects when discussing available treatments. Individualized treatment should consider all of these factors and result in shared decision making between the woman and her healthcare provider.
Expectant management
If fibroids are causing no symptoms and/or were an incidental finding on ultrasound, if they are causing mild symptoms, or if the woman declines medical or surgical treatment, expectant management is an option. Fibroids often regress with menopause, so expectant management may be a viable option for women who are approaching menopause.10 Women who initially choose expectant management should be encouraged to report any change in symptoms such as increasing pain, heavy bleeding, or pelvic pressure. Healthcare providers should evaluate all women with heavy bleeding for anemia and reevaluate the need for medical or surgical intervention based on reported symptoms and clinical presentation. There are no published evidence-based guidelines for how often women should be followed with ultrasound or pelvic exams, although an annual evaluation has been suggested.1,11
 Medical options
Medical options
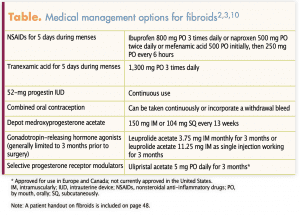
Multiple medical options exist for the management of symptoms associated with fibroids (Table).2,3,10 Dysmenorrhea and HMB are two of the most common complaints. For women who primarily report dysmenorrhea and heavier menses, nonsteroidal anti-inflammatory drugs (NSAIDs) can be taken during menses to reduce discomfort and bleeding. Tranexamic acid, an oral antifibrinolytic, can be taken for 5 days during menstrual bleeding to decrease menstrual blood loss.11 This treatment can have the potential to cause thrombotic events, however, and is therefore not appropriate for women with active thromboembolic disease, a history of thromboembolism, or intrinsic risk of thromboembolism. Due to the increased risk of thrombosis, tranexamic acid should not be combined with estrogen-containing contraception.
Hormonal options exist for the management of fibroid symptoms that also provide contraception.3,11–14 Most of these options, however, are used off label to treat the symptoms associated with fibroids and are not approved by the US Food and Drug Administration (FDA) for that purpose. Progestin-containing intrauterine devices (IUDs) that contain 52 mg of levonorgestrel (LNG) reduce heavy bleeding and decrease dysmenorrhea. The LNG-intrauterine system 20 with 52-mg LNG is FDA approved for the medical treatment of HMB. Expulsion of IUDs is higher among women with fibroids and if fibroids distort the uterine cavity, IUD placement may be challenging or contraindicated.3,11,12 Depot medroxyprogesterone acetate (DMPA) will decrease bleeding and possibly induce amenorrhea, thus controlling some of the most bothersome fibroid symptoms.3 DMPA may reduce bone mineral density (BMD), however, and decisions on the length of treatment will need to be made individually. Combined hormonal oral contraceptive pills are also an option to control bleeding and discomfort. A main disadvantage of all of these options is that they provide symptom management but do not reduce the size of fibroids.3 Thus, although these therapies may help control HMB and dysmenorrhea, bulk symptoms are unaffected.11–13
Gonadotropin-releasing hormone (GnRH) agonists induce amenorrhea, produce a hypoestrogenic state, and reduce uterine volume, including the size of fibroids. Leuprolide acetate is most commonly used. Due to the hypoestrogenic adverse effects of bone loss and vasomotor symptoms, treatment is limited to 3 to 6 months.10,11 Typically, GnRH agonists are used concurrently with iron therapy for 3 months prior to surgery to correct anemia and reduce fibroid bulk to improve surgical outcomes. If they are used for an additional 3 months, norethindrone acetate 5 mg orally once daily is recommended to correct some of the hypoestrogenic effects, including decreased BMD.10,14
Selective progesterone receptor modulators (SPRMs), such as ulipristal acetate, are widely used in Canada and Europe but have yet to receive approval in the United States. SPRMs work by acting as agonists or antagonists on progesterone receptors. They have a direct effect on the endometrium and modulate progesterone pathways that are involved with fibroid growth.12,14–16 Outside of the United States, SPRMs are used preoperatively to control bleeding, correct anemia, and decrease fibroid bulk prior to surgery.12
Surgical options
There are several surgical options for the management of fibroids for women who have severe symptoms and/or have not responded to expectant management or medical treatment. These include hysterectomy, laparoscopic or abdominal myomectomy, uterine artery embolization, and ablation by high-intensity focused ultrasound.1 Decision making in regard to surgical management should include a discussion of the woman’s fertility status, whether she wants to preserve fertility, consideration of preserving the uterus, and past medical and surgical history as well as quality-of-life outcomes.1,3,11
Hysterectomy provides a definitive cure, complete symptom relief, and improved quality of life for women who do not wish to retain their uterus, have no fertility preservation concerns, and are appropriate candidates for surgery. Hysterectomy is the second most common surgical procedure in the United States, with approximately 600,000 performed annually.17 Approximately 90% of hysterectomies are performed due to benign conditions, and fibroid symptoms account for approximately 30% of these cases.7 Hysterectomy may be performed laparoscopically, vaginally, or abdominally depending on uterine and fibroid size. Vaginal hysterectomy is the most common and the preferred approach.13 It offers significant advantages over laparoscopic and abdominal procedures including shorter surgical time, decreased blood loss, decreased risk of paralytic ileus, decreased length of hospital stay, as well as lower overall healthcare costs.18 Vaginal hysterectomy is not appropriate when fibroids or the overall uterine size are very large.2
Alternatively, hysterectomy may be performed laparoscopically (with or without robotic assistance) or as a laparoscopically assisted vaginal procedure. Both vaginal hysterectomy and laparoscopic procedures are considered minimally invasive surgical approaches due to the small abdominal incision, shorter hospital stays, and decreased recovery time.19 Laparoscopic procedures for hysterectomy are increasingly common, rising from 26.1% in 2010 to 43.4% in 2013, with many of these procedures shifting to outpatient surgery.20 Additionally, morcellation during laparoscopic hysterectomy may be performed. Morcellation allows the uterus to be cut into small pieces by a rotating blade before extraction. This procedure, however, is used sparingly due to concerns about iatrogenic dissemination of benign and malignant tissue. The FDA has recommended limiting the use of morcellation techniques to women who are not candidates for en-bloc uterine resection.21 This would include women with large or obstructive fibroids, a significantly enlarged uterus, and women with abdominal adhesions.2,22 The American College of Obstetricians and Gynecologists (ACOG) considers morcellation to be an option for women who have received informed consent but recommends against its use in women with known or suspected uterine cancer.22
Removal of fibroids may also be done by myomectomy (ie, surgical excision of fibroids and uterine reconstruction) for women seeking to preserve their uterus and/or fertility. It may be performed by laparotomy or laparoscopy depending on the number, size, and location of the fibroids. A recent meta-analysis of research found that laparoscopic myomectomies were associated with less postoperative pain, lower postoperative febrile morbidity, shorter hospital stays, and greater full recuperation by postoperative day 15.23
Uterine artery embolization (UAE) is a minimally invasive interventional radiologic procedure in which occluding agents are injected into the uterine arteries causing ischemic necrosis to the uterus and fibroids. This option is available for women seeking to preserve their uterus but is not appropriate for women who wish to preserve their fertility. UAE can be highly effective for treatment of symptoms, but women undergoing this procedure are at increased risk for reoperation (15%–32% within 2–5 years) compared to hysterectomy and myomectomy (7%).13 In randomized controlled trials, UAE has been shown to improve quality of life similar to surgery results but with shorter hospitalization and earlier resumption of daily activities.24 Complications associated with this procedure include risk of infection and abdominal pain due to ischemic necrosis of fibroids. In addition, UAE is contraindicated in women desiring future pregnancies due to ovarian reserve and myometrium compromise.12,13 In a recent systematic review examining UAE and fertility, researchers found that only 50% of women achieved pregnancy after UAE compared to 78% who had a myomectomy.25
High-frequency magnetic resonance–guided focused ultrasound surgery (MRgFUS) is a minimally invasive procedure that uses MRI to target and destroy fibroid tissue using thermal ablation.26 Theoretically, damage to surrounding tissue should be minimal, but a small risk of injury to surrounding structures cannot be excluded.27,28 The use of this procedure is limited by desire for future fertility, presence of intracavitary fibroids, large fibroid volume, and insurance coverage.29 MRgFUS is well tolerated by women, although complaints about heavy bleeding and localized pain can occur.2,30
Practice implications
Women who are diagnosed with fibroids have multiple options for treatment that range from expectant management to hysterectomy. A woman’s age, severity of symptoms, and whether she wishes to preserve her fertility often guide the conversation about which treatment is most appropriate. Women in the fourth decade of life who are expected to transition to menopause may choose a less aggressive approach, as fibroids regress with declining estrogen and progesterone levels of menopause. Nurse practitioners (NPs) can manage the care of women who choose a medical or expectant option. Many noninvasive medical options exist, and based on a women’s symptoms, treatment can be initiated with inexpensive therapy such as NSAIDs and response to treatment evaluated. Regardless of the medical option, all women with fibroids who report HMB should have a complete blood count and ferritin level measured to assess for anemia.31,32 Correction of anemia with oral iron therapy is important, especially if a woman eventually chooses to have surgery. Additionally, endometrial biopsy is indicated if there is sonographic evidence of endometrial hyperplasia or prolonged, erratic, or heavy bleeding is concerning in regard to the possibility of malignancy.32
If women have completed childbearing and/or are experiencing multiple symptoms, a surgical treatment may be an appropriate option. Hysterectomy will bring a definitive end to all fibroid symptoms. Complicated cases and surgical approaches require consultation with physician colleagues, but NPs who care for women with fibroids can provide guidance and clarification on all available options, answer questions, and provide anticipatory guidance about recovery. Although care will be comanaged, NPs can remain an integral member of the healthcare team.
The two primary risk factors for fibroids, advancing age and race, are nonmodifiable. Other modifiable lifestyle factors such as obesity, diet, physical activity, and stress have been associated with the risk of developing fibroids.9 These associations have been identified retrospectively after a woman has been diagnosed with fibroids, however, and how much each individual factor contributes to fibroid development is unknown. Although recommending a diet low in processed foods and high in fruits and vegetables, encouraging regular physical activity, maintaining a normal BMI, and reducing stress are appropriate interventions for all women, these actions are not a guarantee against the development of fibroids.33
Fibroids are often asymptomatic. If symptoms occur, HMB is the most common. The increase in bleeding is often gradual and insidious, however, and women may not immediately recognize that bleeding is heavier.32 Additionally, they may believe that the increased bleeding is a normal part of the menstrual cycle, especially as they approach perimenopause. During preventive healthcare visits, NPs should inquire about menstrual bleeding, any changes in bleeding patterns, and other symptoms associated with fibroids such as increased dysmenorrhea, dyspareunia, and pelvic pressure.11
Fibroids are estimated to affect between 10% and 20% of women who are pregnant.10 Once pregnancy is established, treatment is deferred until after delivery and fibroid size is monitored with serial ultrasound. Women should be advised to report any contractions, abdominal pain, rhythmic back pain, bleeding, or leaking of fluid. Closer follow-up with more frequent visits, measurement of fundal height, and ultrasound assessments is prudent, especially with larger or multiple fibroids.
Conclusion
Fibroids are benign uterine tumors that affect many women and can significantly impact quality of life, increase financial burden, and contribute to infertility. An array of treatment options exists that can be tailored to a woman’s symptoms and reproductive life plans. NPs are an integral part of the healthcare team for women, including participating in the coordination and management of care. As such, they are well positioned to provide education and assist women in making individualized decisions about their healthcare.
Heidi Collins Fantasia is Associate Professor at the Solomont School of Nursing, Zuckerberg College of Health Sciences at the University of Massachusetts in Lowell, and a board-certified women’s health nurse practitioner. Allyssa L. Harris is Associate Professor, WHNP Program Director, and Department Chair at the William F. Connell School of Nursing at Boston College in Chestnut Hill, Massachusetts, and a practicing women’s health nurse practitioner. The authors state that they do not have a financial interest in or other relationship with any commercial product named in this article.
References
- Pérez-López FR, Ornat L, Ceausu I, et al. EMAS position statement: management of uterine fibroids. Maturitas. 2014;79(1):106-116.
- De La Cruz MS, Buchanan EM. Uterine fibroids: diagnosis and treatment. Am Fam Physician. 2017;95(2):100-107.
- Stewart EA. Clinical practice. Uterine fibroids. N Engl J Med. 2015;372(17):1646-1655.
- Fortin C, Flyckt R, Falcone T. Alternatives to hysterectomy: the burden of fibroids and the quality of life. Best Pract Res Clin Obstet Gynaecol. 2018;46:31-42.
- Marsh EE, Al-Hendy A, Kappus D, et al. Burden, prevalence, and treatment of uterine fibroids: a survey of U.S. women. J Womens Health. 2018;27(11):1359-1367.
- Al-Hendy A, Myers ER, Stewart E. Uterine fibroids: burden and unmet medical need. Semin Reprod Med. 2017;35(6):473-480.
- Khan AT, Shehmar M, Gupta JK. Uterine fibroids: current perspectives. Int J Womens Health. 2014;6:95-114.
- Eltoukhi HM, Modi MN, Weston M, et al. The health disparities of uterine fibroid tumors for African American women: a public health issue. Am J Obstet Gynecol. 2014;210(3):194-199.
- Pavone D, Clemenza S, Sorbi F, et al. Epidemiology and risk factors of uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2018;46:3-11.
- Vilos GA, Allaire C, Laberge PY, et al. The management of uterine leiomyomas. J Obstet Gynaecol Can. 2015;37(2):157-178.
- Stewart EA, Laughlin-Tommaso SK, Catherino WH, et al. Uterine fibroids. Nat Rev Dis Primers. 2016;2:16043.
- Donnez J, Dolmans MM. Uterine fibroid management: from the present to the future. Hum Reprod Update. 2016;22(6):665-686.
- Mas A, Tarazona M, Dasi Carrasco J, et al. Updated approaches for management of uterine fibroids. Int J Womens Health. 2017;9:607-617.
- Lethaby A, Puscasiu L, Vollenhoven B. Preoperative medical therapy before surgery for uterine fibroids. Cochrane Database Syst Rev. 2017;11:CD000547.
- Bouchard P, Chabbert-Buffet N. The history and use of the progesterone receptor modulator ulipristal acetate for heavy menstrual bleeding with uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2017;40:105-110.
- Donnez J, Courtoy GE, Donnez O, Dolmans MM. Ulipristal acetate for the management of large uterine fibroids associated with heavy bleeding: a review. Reprod Biomed Online. 2018;37(2):216-223.
- Doll KM, Dusetzina SB, Robinson W. Trends in inpatient and outpatient hysterectomy and oophorectomy rates among commercially insured women in the United States, 2000-2014. JAMA Surg. 2016;151(9):876–877.
- Sesti F, Cosi V, Calonzi F, et al. Randomized comparison of total laparoscopic, laparoscopically assisted vaginal and vaginal hysterectomies for myomatous uteri. Arch Gynecol Obstet. 2014;290(3):485-491.
- Committee on Gynecologic Practice. Committee opinion no 701: choosing the route of hysterectomy for benign disease. Obstet Gynecol. (2017);129(6):e155-e159.
- Morgan DM, Kamdar NS, Swenson CW, et al. Nationwide trends in the utilization of and payments for hysterectomy in the United States among commercially insured women. Am J Obstet Gynecol. 2018;218(4):425.e1-425.e18.
- US Food and Drug Administration. FDA updated assessment of the use of laparoscopic power morcellators to treat uterine fibroids. December 2017. https://www.fda.gov/media/109018/.
- ACOG committee opinion no. 770: uterine morcellation for presumed leiomyomas. Obstet Gynecol. 2019;133(3):e238-e248.
- Bhave Chittawar P, Franik S, Pouwer AW, Farquhar C. Minimally invasive surgical techniques versus open myomectomy for uterine fibroids. Cochrane Database Syst Rev. 2014;10:CD004638.
- Gupta JK, Sinha A, Lumsden MA, Hickey M. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst Rev. 2014;12:CD005073.
- Karlsen K, Hrobjartsson A, Korsholm M, et al. Fertility after uterine artery embolization of fibroids: a systematic review. Arch Gynecol Obstet. 2018;297(1):13-25.
- Fisher K, McDannold NJ, Tempany CM, et al. Potential of minimally invasive procedures in the treatment of uterine fibroids: a focus on magnetic resonance-guided focused ultrasound therapy. Intl J Womens Health. 2015;7:901-912.
- Clark NA, Mumford SL, Segars JH. Reproductive impact of MRI-guided focused ultrasound surgery for fibroids: a systematic review of the evidence. Cur Opin Obstet Gynecol. 2014;26(3):151-161.
- Kim HK, Kim D, Lee MK, et al. Three cases of complications after high-intensity focused ultrasound treatment in unmarried women. Obstet Gynecol Sci. 2015;58(6):542-546.
- Zupi E, Centini G, Sabbioni L, et al. Nonsurgical alternatives for uterine fibroids. Best Pract Res Clin Obstet Gynaecol. 2016;34:122-131.
- Stewart EA, Gostout B, Rabinovici J, et al. Sustained relief of leiomyoma symptoms by using focused ultrasound surgery. Obst Gynecol. 2007;110(2 Pt 1):279-287.
- Friedman AJ, Shander A, Martin SR, et al. Iron deficiency anemia in women: a practical guide to detection, diagnosis, and treatment. Obstet Gynecol Surv. 2015;70(5):342-353.
- Nelson AL, Ritchie JJ. Severe anemia from heavy menstrual bleeding requires heightened attention. Am J Obstet Gynecol. 2015;213(1):97.e1-97.e6.
- Stewart EA, Cookson CL, Gandolfo RA, Schutze-Rath R. Epidemiology of uterine fibroids: a systematic review. BJOG. 2017;124(10):1501-1512.