
MJ, a 31-year-old Hispanic man, presents to the family planning clinic with his wife of 4 years, concerned because they have been trying to conceive for the last 16 months without any success. His wife had her annual well-woman exam with a nurse practitioner (NP) at the clinic 4 months ago. Her physical examination was normal, and she is in good health with regular menses and positive monthly ovulation detection with over-the-counter kits. MJ, on the other hand, has not seen a provider for any examination for at least 5 years.
MJ describes occasionally feeling a small lump on his left testicle accompanied by intermittent pain described as a dull ache for the “last few years” with occasional sharp fleeting pain about once a month. He says he has never fathered a child and is worried that he might have a problem that is preventing him and his wife from being able to get pregnant.
Because MJ’s wife was comfortable with the NP that she saw for her annual well-woman visit, they ask to see her. This NP is a women’s health nurse practitioner (WHNP). Will this WHNP be able to see a male patient for this concern? It is a common misconception that WHNPs only care for the sexual and reproductive health (SRH) care needs of women. In the 2018 Women’s Health Nurse Practitioner Workforce Demographics and Compensation Survey, 24% of respondents reported caring for the SRH needs of men.1 A recent Nurse Practitioner in Women’s Health (NPWH) position statement affirms the role of WHNPs in the evaluation and management of common SRH problems in men.2 The NPWH WHNP guidelines for practice and education outline specific male SRH competencies and curriculum content.3 Finally, the national certifying body of WHNPs, the National Certification Corporation, has included questions and content on male SRH for over 2 decades. Thus, the WHNP is qualified to see men for initial evaluation of fertility and testicular mass or pain.
- Medical history: childhood illnesses, diabetes, cancer, hypertension, mental health
- Surgical history: surgery or trauma to the pelvic area
- Medication reconciliation: including supplements, over-the-counter treatments, as well as any allergies
- Review of systems: genitourinary (dysuria or pelvic pain), lymphatics (pelvic lymph nodes), gastrointestinal, muscular, endocrine, and psychiatric (depression or anxiety) to rule out other differential diagnoses
Health history
The health history is conducted in a private room, while the patient is fully clothed to facilitate a comfortable environment. For concerns regarding fertility and/or testicular lump or pain, components of a focused health history include medical conditions, surgeries, medications, environmental and occupational gonadotoxic exposures including heat, and a review of systems to provide direction in developing a differential diagnosis. Topics to include in this first part of the health history are provided in Box 1.4 Prior to completing the substance use, sexual, and reproductive portions of the health history, the clinician should let the patient know that some of the questions asked may seem of a personal nature. Explaining that this information is essential to determine the cause of testicular pain and factors that may be affecting fertility fosters open communication. A nonjudgmental approach is critical. The substance use assessment includes smoking, vaping, alcohol, recreational drugs, and any prescription medications used for other than medically intended purposes (eg, opioids, anabolic steroids, testosterone). The sexual and reproductive history includes sexual practices, partners, history of sexually transmitted infections, libido, ability to have and maintain an erection, ability to ejaculate, any pain during sex, and family history of infertility.
MJ has no significant medical or surgical history and takes no medications. He works as an accountant and plays baseball on the weekend with friends. He has no known toxic exposures. MJ does not smoke, vape, or use recreational drugs. He drinks 2 to 3 beers on the weekends. He and his wife have vaginal and oral sex once or twice each week. He does not have problems with arousal, erection, or ejaculation. MJ states he did have gonorrhea when he was about age 23 years that was treated without any complications. There is no known family history of infertility of which he is aware.
MJ expresses having a fullness of the left testicle, which sometimes is accompanied by pain that ranges from dull to sharp without radiation. He expresses that occasionally he has an intermittent feeling of a sudden “flick” or sharp pain to the testicle lasting only a few seconds. He states these symptoms are exacerbated with prolonged standing and when he bears down. Prior to the last few years, he states he has never had any issues with his testicle, including during adolescence. He denies any symptoms with the right testicle.
Physical examination
Blood pressure and height and weight for body mass index should be assessed. If indicated by patient age or health history, other physical examination components may be included. The patient is provided with a drape to cover the groin area and can keep his underwear on until this portion of the examination begins. The clinician explains to the patient that the examination will include inspection and palpation of the penis, urethral opening, scrotum, and testicles. If the patient is anxious, providing instruction on slow, deep breathing will assist in relaxation. The patient usually stands for the examination of the genitals and groin with the clinician seated on a chair or stool. The male genital exam includes the following4:
• Inspection of the penis noting location of the urethral meatus and any discharge or skin changes
• Inspection and palpation of scrotum and both testes; noting size, any nodules, and tenderness, as well as presence and consistency of vas deferens and epididymis
• Palpation of inguinal lymph nodes for enlargement and/or tenderness
The scrotal exam begins with an inspection of the skin and scrotal contours for visible swelling, masses, or veins. The testis, epididymis, and spermatic cord on each side are palpated starting at the superior posterior surface of the testis and progressing downward. Pressure on the testes normally produces some discomfort. Assessment for a scrotal mass includes asking the patient to bear down (Valsalva maneuver) while standing. Any scrotal mass should be assessed with the patient in both standing and supine positions. See Table 1.
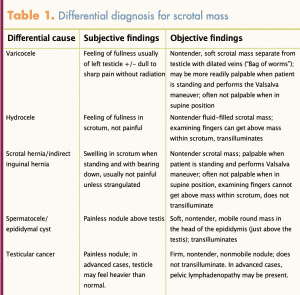
Varicocele and male infertility
The WHNP noted a nontender soft mass (sometimes described as feeling like a bag of worms) in the left scrotal area separate from the testicle when MJ was standing and performed the Valsalva maneuver. The mass disappeared when MJ changed to a supine position. These examination findings are consistent with varicocele. Varicoceles found on physical examination are graded as grade 3 when visible on inspection, grade 2 when felt with easy palpation, and grade 1 when only palpable with Valsalva maneuver.5 Significantly, only palpable varicoceles have been associated with infertility.6 There were no other abnormal examination findings.
A varicocele is an abnormal dilation of the spermatic veins. It is commonly due to the abnormal dilation of the pampiniform plexus (approximately 10 veins draining the testis and epididymis), surrounds the testicular artery in the spermatic cord, and lies anterior to the ductus deferens. Varicoceles affect 15% of the general male population.6 They often initially manifest in adolescent males and increase in size and symptoms with age, but they frequently are not discovered until the patient has a workup for infertility or unmanageable pain. Varicoceles can impair sperm production and function, resulting in infertility. Studies have shown that as many as 41% of all males who experience primary infertility have a varicocele, along with up to 81% of males who are seeking care for secondary infertility or infertility after one has conceived prior.7,8 The exact pathophysiology of the varicocele in infertility is unknown. Some possible causes, however, could be related to elevated temperature, venous stasis and reflux, and low intra-testicular testosterone.9 Other causes of male infertility should be included in the evaluation. Common causes for male infertility are listed in Box 2.10
- Low sperm count and/or poor sperm quality
- Congenital abnormalities
- Hormone imbalance
- Genetic deficits
- History of cardiac, renal, and metabolic conditions
- Lifestyle factors, such as tobacco, alcohol, and medication and illicit drug use
- Certain types of environmental exposures
Diagnostic testing
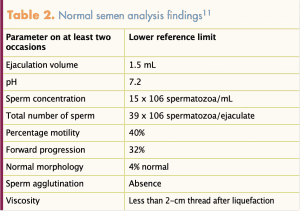
Not all individuals with a varicocele have inadequate sperm; therefore, to determine the extent that MJ’s varicocele is the root cause of infertility, the patient should have a semen analysis. Table 2 lists normal semen analysis findings.11 Prior to the analysis, the patient must remain abstinent for at least 2 days. The specimen is usually obtained by masturbation and collecting all contents into a specimen cup provided by the clinic. Due to the sensitive timing, it is highly recommended that this occurs within an environment that has an andrology laboratory available on site. It can also be done at home, but the specimen must be kept warm and taken to the lab within 1 hour of collection. The patient should be instructed that the typical ejaculation volume is 1.5 mL, so it is not expected to fill the cup. MJ’s semen analysis results included a low volume with normal motility and normal forms. An abnormal semen analysis requires repeat specimen collection about 4 to 6 weeks after the initial analyses related to highly established inner variability of male sperm production. MJ’s repeat semen analysis produced the same results as the initial test.
 Since MJ is also having pain, imaging via a scrotal ultrasound should be ordered. Color Doppler ultrasound (CDUS) is the gold standard for imaging assessment of varicoceles.12 An ultrasound can help the provider rule out solid mass, assess the extent of damage to the testicular parenchyma, determine the need and candidacy for surgical treatment options, and assist the surgeon in predicting the effects of therapy.13 Ultrasound provides a measurement of venous dilations and reflux in the pampiniform plexus in real time, allowing for higher sensitivity and specificity than a physical exam alone.14 This test is noninvasive and relatively painless. A typical report that is positive for varicocele would include the degree of reflux assessed by CDUS grading 1 (no varicosities seen with Valsalva) through 5 (spontaneous reflux at rest with no Valsalva) classification system.12 This form of imaging demonstrates high accuracy, with sensitivity and specificity near 100%.12 MJ’s ultrasound report interpreted a grade 3 varicocele of the left testis.
Since MJ is also having pain, imaging via a scrotal ultrasound should be ordered. Color Doppler ultrasound (CDUS) is the gold standard for imaging assessment of varicoceles.12 An ultrasound can help the provider rule out solid mass, assess the extent of damage to the testicular parenchyma, determine the need and candidacy for surgical treatment options, and assist the surgeon in predicting the effects of therapy.13 Ultrasound provides a measurement of venous dilations and reflux in the pampiniform plexus in real time, allowing for higher sensitivity and specificity than a physical exam alone.14 This test is noninvasive and relatively painless. A typical report that is positive for varicocele would include the degree of reflux assessed by CDUS grading 1 (no varicosities seen with Valsalva) through 5 (spontaneous reflux at rest with no Valsalva) classification system.12 This form of imaging demonstrates high accuracy, with sensitivity and specificity near 100%.12 MJ’s ultrasound report interpreted a grade 3 varicocele of the left testis.
Treatment
Surgical treatment of a varicocele that is causing impaired sperm production is indicated if the patient currently desires to conceive or plans to conceive in the future. Patients who are symptomatic, usually with pain or reduced testicular size, are also candidates for surgical intervention. Surgery by way of dilating the veins of the pampiniform plexus is currently the gold standard for treatment for a varicocele when fertility is desired to improve venous drainage.15 It has over a 90% success rate with minimal complications.6 This correction has a direct correlation to increased sperm concentration and the overall motility in males with a higher grade of varicocele.5 Surgery usually only takes 30 minutes and is outpatient, with full recovery occurring in 2 to 3 weeks. Lifting restrictions are very short term. Another option is a percutaneous embolism, which is a procedure using metal coils to obstruct the dilated spermatic veins done by an interventional radiologist. With this procedure, there is a small risk of recurrence, but this is dependent on the technique and how the coils were placed.16 There are currently no effective medical treatments available.15 Experimental studies are in progress with antioxidant therapy, but this is not currently approved for treatment.17 Patients who have impaired but not absent sperm production who are not candidates for surgery or prefer not to have surgery may consider intrauterine insemination or in vitro fertilization to conceive. MJ is referred to a urologist for a surgery consult to obtain more information on the surgical procedures available for him related to his testicular pain and the primary infertility. It is important to note that even if his semen analysis would have been normal, a referral should still be made to evaluate the testicular pain and explore surgical options for relief. Untreated varicoceles can cause increased pain to the patient over time, testicular atrophy, and future infertility.8
Implications for practice
This case study is an exemplar of a male patient the WHNP may see in a primary or specialty care setting for SRH care. WHNPs are equipped with the appropriate knowledge, skills, and abilities to conduct an initial evaluation for male infertility, including an assessment for a varicocele. A patient with a varicocele can often be diagnosed in the office through a focused health history and physical examination. The WHNP can order and interpret semen analyses and a scrotal ultrasound if indicated. Although a referral is necessary for treatment, WHNPs play a pivotal role as the first point of contact for patients with infertility concerns. Continuing education opportunities to update knowledge and skills for providing male SRH can build more confidence in the ability to provide this service that is within the WHNP role and scope of practice.
Randee L. Masciola is Assistant Professor of Clinical Nursing at the Ohio State University, College of Nursing, in Columbus, Ohio. She is also on the editorial advisory board for Women’s Healthcare: A Clinical Journal for NPs. Justin M. Waryold is Clinical Assistant Professor in the School of Nursing at Stony Brook University in Stony Brook, New York. The authors state that they do not have a financial interest in or other relationship with any commercial product named in this article.
References
- National Association of Nurse Practitioners. 2018 Women’s Health Nurse Practitioner Workforce Demographics and Compensation Survey: Highlights Report. November 12, 2019. Women’s Healthcare Clin J NP. https://www.npwomenshealthcare.com/2018-npwh-womens-health-nurse-practitioner-workforce-demographics-and-compensation-survey-highlights-report/.
- National Association of Nurse Practitioners in Women’s Health. Position statement on male sexual and reproductive health—the role of Women’s Health Nurse Practitioners. Women’s Healthcare Clin J NP. 2018;6(4):18-21.
- National Association of Nurse Practitioners in Women’s Health. Women’s Health Nurse Practitioner: Guidelines for Practice and Education. 8th ed. Washington, DC: NPWH; 2020.
- Marcell AV; Male Training Center for Family Planning and Reproductive Health. Preventive Male Sexual and Reproductive Health Care: Recommendations for Clinical Practice. Philadelphia, PA: Male Training Center for Family Planning and Reproductive Health and Rockville, MD: Office of Population Affairs; 2014.
- Asafu-Adjei D, Judge C, Deibert CM, et al. Systematic review of the impact of varicocele grade on response to surgical management. J Urol. 2020;203(1):48-56.
- Practice Committee of the American Society for Reproductive Medicine; Society for Male Reproduction and Urology. Report on varicocele and infertility: a committee opinion. Fertil Steril. 2014;102(6):1556-1560.
- Alsaikhan B, Alrabeeah K, Delouya G, Zini A. Epidemiology of varicocele. Asian J Androl. 2016;18(2):179-181.
- Gordhan CG, Sadeghi-Nejad H. Scrotal pain: evaluation and management. Korean J Urol. 2015;56(1):3-11.
- Agarwal A, Sharma RK, Desai NR, et al. Role of oxidative stress in pathogenesis of varicocele and infertility. Urology. 2009;73(3):461-469.
- Leaver RB. Male infertility: an overview of causes and treatment options. Br J Nurs. 2016;25(18):S35-S40.
- Practice Committee of the American Society for Reproductive Medicine. Diagnostic evaluation of the infertile male: a committee opinion. Fertil Steril. 2015;103(3):e18-e25.
- Pauroso S, Di Leo N, Fulle I, et al. Varicocele: ultrasonographic assessment in daily clinical practice. J Ultrasound. 2011;14(4):199-204.
- Lorenc T, Krupniewski L, Palczewski P, Golebiowski M. The value of ultrasonography in the diagnosis of varicocele. J Ultrason. 2016;16(67):359-370.
- Kwak N, Siegel D. Imaging and interventional therapy for varicoceles. Curr Urol Rep. 2014;15(4):399.
- Butler C, Ellsworth P. Contemporary approach to diagnosis, management, and treatment of varicocele in the adolescent. Urol Nurs. 2014;34(6):271-280.
- Sheehan M, Briody H, O’Neill DC, et al. Pain relief after varicocele embolization: the patient’s perspective. J Med Imaging Radiat Oncol. 2020 Feb 11. [Online ahead of print.]
- Garg H, Kumar R. An update on the role of medical treatment including antioxidant therapy in varicocele. Asian J Androl. 2016;18(2):222-228.