
Faculty
Nancy R. Berman, MSN, ANP-BC, NCMP, FAANP, is a nurse practitioner at Michigan Healthcare Professionals in Farmington Hills and a Clinical Instructor in the Department of Obstetrics and Gynecology at Wayne State University School of Medicine in Detroit, both in Michigan.
Intended audience
This continuing education (CE) activity has been designed to meet the educational needs of nurse practitioners, certified nurse-midwives, and other advanced practice clinicians who care for women.
CE approval period
Now through May 31, 2017
Estimated time to complete this activity
1 hour
CE approval hours
1.0 contact hour of CE credit, including 1.0 contact hour of pharmacology content
Needs assessment
Most cervical cancers are preventable. The incidence of cancer related to HPV infection has declined significantly since the inauguration of screening programs in the U.S. more than 50 years ago. However, too many women are still developing cervical cancer, and 4,400 are dying of it each year. More cases of cervical cancer could be prevented with increased uptake of HPV vaccination, increased addition of HPV testing in screening, and improved access to cervical cancer screening in under-screened and unscreened populations.
Goal statement
Nurse practitioners and other advanced practice clinicians who care for women will make a strong recommendation that children aged 11 or 12 get fully immunized against HPV so as to prevent HPV-related diseases in the future.
Educational objectives
At the conclusion of this educational activity, participants should be able to:
1. Understand the efficacy, safety, and immunogenicity of the HPV vaccine, including the new 9-valent vaccine.
2. Be familiar with all of the ACIP guidelines for the HPV vaccine.
3. Boost HPV vaccine uptake in their patient population.
Accreditation statement
This activity has been evaluated and approved by the Continuing Education Approval Program of the National Association of Nurse Practitioners in Women’s Health (NPWH), and has been approved for 1.0 contact hour of CE credit, including 1.0 contact hour of pharmacology content.
Faculty disclosures
NPWH policy requires all faculty to disclose any affiliation or relationship with a commercial interest that may cause a potential, real, or apparent conflict of interest with the content of a CE program. NPWH does not imply that the affiliation or relationship will affect the content of the CE program. Disclosure provides participants with information that may be important to their evaluation of an activity. Faculty are also asked to identify any unlabeled/unapproved uses of drugs or devices made in their presentation.
Nancy R. Berman, MSN, ANP-BC, NCMP, FAANP, has disclosed that she has financial relationships with Hologic and Shionogi.
Disclosure of unlabeled use
NPWH policy requires authors to disclose to participants when they are presenting information about unlabeled use of a commercial product or device or an investigational use of a drug or device not yet approved for any use.
Disclaimer
Participating faculty members determine the editorial content of the CE activity; this content does not necessarily represent the views of NPWH or Merck & Co., Inc. This content has undergone a blinded peer review process for validation of clinical content. Although every effort has been made to ensure that the information is accurate, clinicians are responsible for evaluating this information in relation to generally accepted standards in their own communities and integrating the information in this activity with that of established recommendations of other authorities, national guidelines, FDA-approved package inserts, and individual patient characteristics.
Successful completion of this activity
Successful completion of this activity, J-16-02, requires participants to:
1. “Sign In” at the top right-hand corner of the website if you have an NPWH account. You must be signed in to receive credit for this course. If you do not remember your username or password, please follow the “Forgot Password” link and instructions on the sign-in page. If you do not have an account, please click on “Create an Account.”
2.Read the learning objectives, disclosures, and disclaimers on the next page.
3.Check “Agree to Terms” on the next page and then click the “Continue” button.
4. Study the material in the learning activity during the approval period (now through May 31, 2017).
5.Complete the posttest and evaluation. You must earn a score of 70% or better on the posttest to receive CE credit.
6.Print out the CE certificate if successfully completed.
Commercial support
This activity is supported by educational grants from Merck & Co., Inc.
Before reading the article, click here to take the pretest.
Cervical cancer, caused in nearly all cases by human papillomavirus (HPV), is considered a vaccinepreventable disease. Anogenital warts and other forms of cancer can also be caused by HPV, and can be reduced in frequency with HPV vaccination. Despite the proven efficacy and safety of the three available HPV vaccines—one of which targets up to nine different HPV genotypes—only about one-third of girls in the United States have received the three recommended doses. The author reviews information about the HPV vaccines and the guidelines for their use, and offers strategies for healthcare providers to implement in order to improve HPV vaccine uptake in their age-appropriate patients.
Human papillomavirus (HPV) infection is the most common sexually transmitted infection in the United States.1 Almost all sexually active adults are or will be infected by HPV at some point in their lives, even if they have had sex with only one other person. Although the vast majority of HPV infections are asymptomatic and resolve spontaneously, a few persist and can lead to cancer.2 Persistent infections with oncogenic HPV types can cause cancers of the cervix, vulva, vagina, anus, and penis, as well as the oropharynx. Infection with non-oncogenic HPV types can cause anogenital warts.
About 79 million persons in the U.S. are already infected with HPV, and 14 million persons acquire HPV infection each year.3 An estimated 17,600 women and 9,300 men receive a diagnosis of an HPVrelated cancer each year. For U.S. women, cervical cancer is the most common HPV-related cancer; approximately 11,000 women are diagnosed with it annually and 4,400 women die of it. For U.S. men, oropharyngeal cancer is the most common HPV-related cancer; about 7,200 U.S. men are diagnosed with it each year.
In an Annual Report to the Nation on the Status of Cancer, Jemal et al4 reported that many types of HPV-related cancers were on the rise, some disproportionately affecting certain racial and ethnic minorities. For example, from 2000 to 2009, oral cancer rates increased 4.9% for Native American men, 3.9% for white men, 1.7% for white women, and 1% for Asian men. Anal cancer rates doubled from 1975 to 2009. Vulvar cancer rates rose for white women and African-American women and penile cancer rates increased among Asian men.
Most cervical cancers are preventable. The incidence of this disease has declined significantly since the inauguration of screening programs in the U.S more than 50 years ago.5 However, too many women are still developing cervical cancer, and 4,400 are dying of it each year. More cases of cervical cancer could be prevented with increased uptake of HPV vaccination, increased addition of HPV testing in screening, and improved access to cervical cancer screening in under-screened and unscreened populations.
HPV vaccines
For decades, the best that healthcare providers (HCPs) could offer patients in terms of lowering their risk for developing HPV-related cancers were screenings for cervical cancer precursors and for anal pre-cancers and cancers (in highrisk populations) and inspection for vulvar pre-cancers and cancers. But in June 2006, the FDA approved the first vaccine to prevent disease caused by any of four HPV genotypes: 6 and 11, which cause anogenital warts; and 16 and 18, which are the most common causes of cervical cancer.6
Three HPV vaccines are on the market in the U.S. (Table).3 The bivalent HPV (2vHPV), quadrivalent HPV (4vHPV) and 9-valent HPV (9vHPV) vaccines each target HPV 16 and 18, the types that cause about 70% of cervical cancers and most other HPV-linked cancers in women and men.3,7 The 9vHPV vaccine targets five additional cancer-causing types (HPV 31, 33, 45, 52, 58), which account for about 15% of cervical cancers. The 4vHPV and 9vHPV vaccines also protect against HPV 6 and 11, the types that cause 90% of anogenital warts.
Efficacy
Clinical trials have suggested that HPV vaccines, if used optimally, could likely prevent most cervical cancers.2 Of 10,000 young women vaccinated as part of clinical trials before they could have been exposed to oncogenic forms of HPV, none developed HPV 16- or 18-associated cervical lesions, which are precursors to invasive cancer.8,9 HPV vaccines have been shown to prevent other HPV 16- or 18-associated anogenital pre-cancers and HPV 6- or 11-associated genital warts with similar efficacy.9,10 Women who received the 2vHPV vaccine as part of a clinical trial had a much lower prevalence of oral HPV infection than did participants who had not received the HPV vaccine.11
In a study reported in March 2016, Markowitz et al12 analyzed 4vHPV type prevalence (i.e., types 6, 11, 16, and 18) in cervicovaginal specimens from females aged 14- 34 years in NHANES (National Health and Nutrition Education Survey) in the pre-vaccine era (2003-2006) and during 4 years of the vaccine era (2009-2012). Within 6 years of HPV vaccine introduction, there was a 64% decrease in 4vHPV type prevalence among females aged 14-19 and a 34% decrease in 4vHPV type prevalence among those aged 20-24 years. There was no decrease in 4vHPV type prevalence in older age groups.
Because the HPV vaccine has been available for only 10 years, it will take a while to assess its efficacy in preventing invasive cancers that take years or decades to develop following persistent infection.
Safety
Three population-based safety studies of the HPV vaccine have been conducted in the U.S.13-15 These studies have identified no serious safety concerns, although one study showed an increased risk of syncope on the day of vaccination and skin infections in the 2 weeks following vaccination.15 Gee et al12 evaluated the risk for venous thromboembolism (VTE) in persons aged 9-26 years, and found no increased risk of VTE following vaccination with the 4vHPV vaccine. Chao et al14 found no association between 4vHPV vaccine use and 16 autoimmune conditions.
According to ongoing safety monitoring by the CDC, most reports of adverse reactions to the vaccine are non-serious.16 Among the 7.6% of reports classified as serious, the most common side effects are headache, nausea, vomiting, and fever. Syncope is a common non-serious problem in both female and male adolescents who receive the HPV vaccine. Of note, syncope is not specific to the HPV vaccine. It is recommended that after receiving the injection, patients remain seated for 15 minutes before leaving the clinical setting.
Impact
Drolet et al17 conducted a systematic review and meta-analysis of 20 studies in 9 high-income countries to assess population-level consequences and herd effects after female HPV vaccination programs and to verify whether the high efficacy reported in randomized controlled trials was materializing in real-world situations. The investigators found that in countries with female vaccination coverage >50%, HPV type 16/18 infections decreased significantly, by 68%, and anogenital warts decreased significantly, by 61%, between pre- and post-vaccination periods in girls aged 13-19 years. In addition, significant reductions were recorded in HPV types 31, 33, and 45 in this age group of girls, suggesting cross-protection. Furthermore, the incidence of anogenital warts declined significantly in boys younger than 20 years and in women aged 20-39 years, suggesting herd effects. In countries with female vaccination coverage <50%, significant reductions in HPV types 16/18 infection and in anogenital warts occurred in girls younger than 20, with no indication of cross-protection or herd effects.
Duration of immunity
According to a 2011 review, the HPV vaccine was found to provide protection against persistent cervical HPV 16/18 infections for up to 8 years—the maximum time of research follow-up at that point.18 More will be known about the total duration of protection as research continues. To date, no evidence suggests waning immunity such as that seen with the menin go coccal conjugate vaccine, which now requires a second dose. Multiple cohort studies are in progress to monitor the duration of immunity.
More about the 9-valent vaccine
To gain the recent endorsement of the CDC’s Advisory Committee on Immunization Practices (ACIP), the 9vHPV vaccine had to demonstrate efficacy, immunogenicity, and safety.19 In particular, the newest vaccine had to show efficacy in terms of preventing infection and disease related to HPV 31, 33, 45, 52, and 58 in a susceptible population and of generating an antibody response to HPV 6, 11, 16, and 18 that was non-inferior to that generated by the 4vHPV vaccine. Studies conducted by Joura et al20 and Luxembourg et al21 showed precisely that.
In 7 pre-licensure studies, the 9vHPV vaccine was evaluated in more than 15,000 females and males.22 In some studies, the 9vHPV vaccine was compared with the 4vHPV vaccine. The 9vHPV vaccine caused slightly more reactions— primarily swelling and redness—at the injection site. As with the 4vHPV vaccine, side effects associated with the 9vHPV vaccine were generally mild. A video summarizing information about the 9vHPV vaccine is available here.
ACIP guidelines
Routine immunizations for 11- and 12-year-olds include HPV vaccination. HCPs should recommend the HPV vaccine on the same day and in the same way as the other vaccines for preteens.
Age, gender, and vaccine type
ACIP recommends that routine HPV vaccination be initiated at age 11 or 12, although the vaccination series can be started as early as age 9.19 Vaccination is also recommended for females aged 13-26 and for males aged 13-21 who have not been vaccinated previously or who have not completed the 3-dose series. HPV vaccination is recommended through age 26 years for men who have sex with men and for immunocompromised persons (including those with HIV infection) who have not been vaccinated previously or have not completed the 3-dose series. Females should receive the 2vHPV, 4vHPV, or 9vHPV vaccine and males should receive the 4vHPV or 9vHPV vaccine. The dosing schedule for each vaccine type is shown in the Table. If the vaccine schedule is interrupted, the vaccination series need not be restarted.
Interchangeability
ACIP recommends that, whenever possible, the HPV vaccination series for females be completed with the same HPV vaccine product.16 If vaccination providers do not know or do not have available the HPV vaccine product previously administered to a given patient, or are in settings transitioning to the 9vHPV vaccine, any available HPV vaccine product may be used to continue or complete the series for females for protection against HPV 16/18, and the 4vHPV or 9vHPV vaccine may be used to continue or complete the series for males.19 There are no data on the efficacy of fewer than 3 doses of 9vHPV.
Concomitant administration with other vaccines
HPV vaccine can be administered at the same visit as other age appropriate vaccines, such as the tetanus/diphtheria/acellular pertussis (Tdap) and quadrivalent meningococcal conjugate vaccines.16 Giving all indicated vaccines togethe at a single visit increases the likelihood that adolescents will receive each vaccine on schedule. Each vaccine should be administered using a separate syringe at a different anatomic site.
History of sexual abuse or assault
The newest vaccination schedule issued by ACIP recommends that the HPV vaccine be given as early as age 9 or 10 if a child has a history of sexual abuse.23 Studies estimate that 1 in 4 girls and 1 in 20 boys will experience sexual abuse before age 18.
HPV vaccine coverage rates
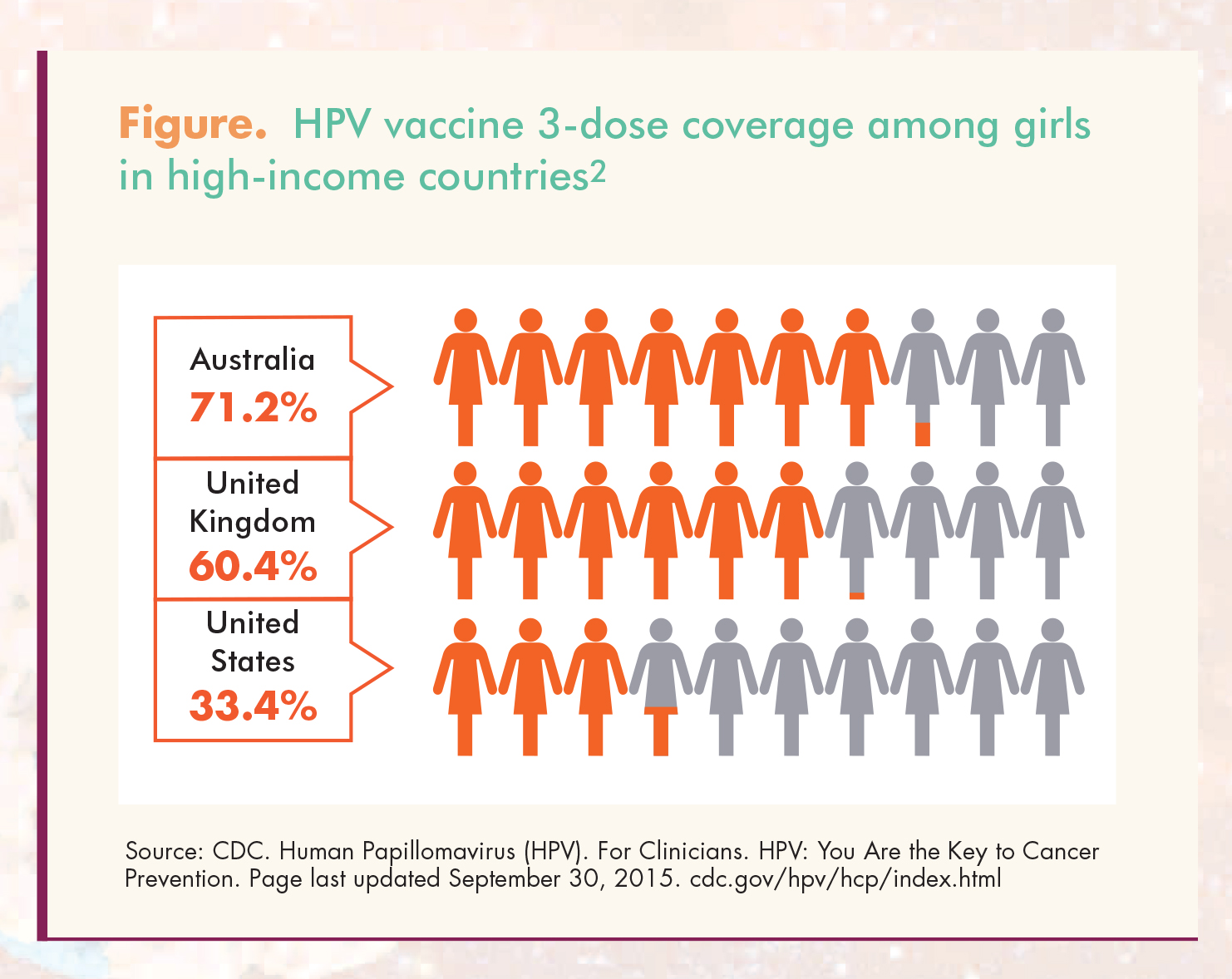
The HPV vaccine has been available for almost 10 years. Despite its proven efficacy and safety, HPV vaccine coverage rates have been low. In 2012, only 53.8% of 13- to 17- year-old girls had received the first HPV vaccine dose and only 33.4% had completed all 3 recommended doses.24 These rates were substantially lower than HPV vaccine coverage rates in other high-income countries such as Australia and the United Kingdom (71.2% and 60.4%, respectively; Figure).2 More recent reports have indicated some improvement in HPV vaccine coverage rates. For example, in 2014, among girls aged 13-17, 60.0% received at least one dose and 39.7% received the 3 recommended doses.25 The improvement was laudable but insufficient: 6 of every 10 girls in this country are not fully vaccinated against HPV.
{kind=link}
Strategies to boost vaccination rates
And, thus, a call to action: Concerted efforts are needed to increase HPV vaccine uptake and achieve its potential to prevent cancers.2 These efforts should promote both initiation of the first dose and completion of all 3 doses for age-eligible adolescents, as well as eligible young adults. What can HCPs do to improve vaccination rates?
1. Keep up to date on what you can do to prevent HPV-related cancers
The CDC launched a new website, HPV: You are the key to cancer prevention, for HCPs so that everything about HPV vaccination is found in one place. The website is easy to navigate; it has only 1 page and 3 tabs: Know the Facts, Commit to the Cause, and Lead the Conversation.26 The recommendations described in items 2, 3, 4, and 6 were also derived from this new CDC website.26
2. Make a strong recommendation
The high coverage rates for the Tdap and meningococcal conjugate vaccines suggest that most preteens and teens are not only going to see their HCP, but they are also getting at least one of the recommended adolescent vaccines.25 However, according to the 2013 National Immunization Survey-Teen, one-third of the parents of girls and more than half of the parents of boys said their child’s HCP had not recommended HPV vaccination—the No. 1 reason for failure to vaccinate their children.27,28 Had the HPV vaccine been administered during visits when another vaccine was given, vaccination coverage for ≥1 dose could have reached 91% by age 13 for adolescent girls born in 2000.25 Evidence shows that an HCP recommendation to get vaccinated is the single most influential factor in determining whether parents gets an immunization for their child!24 HCPs should provide clear and strong recommendations that the HPV vaccine series be given to preteens.
3. Seize the day
Timing is everything.26 Making a strong pitch for preteens to be vaccinated is necessary, but not sufficient. HCPs should take advantage of appropriate opportunities to vaccinate their preteen patients against HPV—for example, during school or camp physical exams—when these patients are still coming in for regular office visits. Once these patients go to college or to work, they are less likely to see their HCP for yearly checkups. To make a timely recommendation, HCPs should do it the same way and the same day that they recommend the Tdap and meningococcal vaccines.
4. Use a reminder system
Reminder systems shown to increase HPV vaccination rates include a reminder letter and direct messaging via automated text, prerecorded voice, and/or postcard.29,30
5. Educate mothers during their routine visits
Another useful strategy is to educate mothers when they are being screened for cervical cancer about the role of HPV infection in cervical cancer. HCPs should explain to mothers that they are undergoing an HPV test to determine whether the virus is present on their cervix, and that their preteen daughters or sons can be vaccinated to be protected from being infected by the HPV types in the vaccine. HCPs can simply say: “HPV is the cause of cervical cancer. We are screening you with the HPV test and the Pap test to detect any existing HPV infection or cervical pre-cancers, which we can then treat to keep them from progressing to cancer. But we can vaccinate your daughters and sons to prevent HPV infection and therefore prevent cervical pre-cancer and cervical cancer.”
6. Address parents’ specific concerns
If a parent’s main concern is side effects, HCPs can say: “Vaccines, like any medication, can have side effects. With the HPV vaccine, the most common side effect is pain and redness at the site of the injection. These symptoms should go away quickly. In addition, the HPV vaccine has not been linked to any serious or long-term side effects.”26 If a parent’s main concern is effect on fertility, HCPs can say, “No scientific data suggest that getting the HPV vaccine has any effect on future fertility. In fact, not getting the HPV vaccine can put a woman’s fertility in jeopardy. Persistent HPV infection can cause cervical cancer, and the treatment of cervical cancer can leave a woman unable to have children. Even treatment for cervical pre-cancer can put a woman at risk for problems with her cervix during pregnancy, causing preterm delivery or other problems.”
7. Hand out written materials
Written materials are helpful in supporting patient education. Patients can refer to them later, after they have spoken to you. Many written materials are available in languages other than English. Spanish-language materials are particularly easy to find. Patient factsheets regarding the HPV vaccine are available on the CDC website.
Conclusion
Considering how effective the HPV vaccine will be in preventing cervical cancer, as well as other HPV-related cancers in both females and males, virtually all preteen girls and boys and all eligible young women and men should be immunized. Vaccination uptake rates, although increasing slowly, are still much too low. These rates will rise dramatically only when HCPs across the country heed the call to action and educate parents about the efficacy and safety of this vaccine and take advantage of opportunities to initiate and complete administration of the 3-dose series.
References
1. Centers for Disease Control and Prevention (CDC). Genital HPV Infection – Fact Sheet. Last updated February 3, 2016.
2. President’s Cancer Panel Annual Report 2012-2013. Accelerating HPV Vaccine Uptake: Urgency for Action to Prevent Cancer.
3. CDC. Clinician Factsheets. HPV Vaccination Information for Clinicians. Page last updated December 29, 2015.
4. Jemal A, Simard EP, Dorell C, et al. Annual Report to the Nation on the Status of Cancer, 1975-2009, featuring the burden and trends in human papillomavirus (HPV)-associated cancers and HPV vaccination coverage levels. J Natl Cancer Inst. 2013; 105(3):175-201.
5. National Cancer Institute. A Snapshot of Cervical Cancer: Incidence and Mortality. November 5, 2014.
6. FDA. June 8, 2006 Approval Letter — Human Papillomavirus Quadrivalent (Types 6, 11, 16, 18) Vaccine, Recombinant.
7. CDC. Clinician Factsheets. Supplemental Information and Guidance for Vaccination Providers Regarding Use of 9- Valent HPV Vaccine. Page last updated December 29, 2015.
8. Lehtinen M, Paavonen J, Wheeler CM, et al. Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-ofstudy analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol. 2012;13(1):89-99.
9. Muñoz N, Kjaer SK, Sigurdsson K, et al. Impact of human papillomavirus (HPV)-6/11/16/18 vaccine on all HPVassociated genital diseases in young women. J Natl Cancer Inst. 2010;102(5):325-339.
10. Palefsky JM, Giuliano AR, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med. 2011; 365(17):1576-1585.
11. Herrero R, Quint W, Hildesheim A, et al. Reduced prevalence of oral human papillomavirus (HPV) 4 years after bivalent HPV vaccination in a randomized clinical trial in Costa Rica. PLoS One. 2013;8(7):e68329.
12. Markowitz LE, Liu G, Hariri S, et al. Prevalence of HPV after introduction of the vaccination program in the United States. Pediatrics. 2016;137(3):1-9.
13. Gee J, Naleway A, Shui I, et al. Monitoring the safety of quadrivalent human papillomavirus vaccine: findings from the Vaccine Safety Datalink. Vaccine. 2011;29(46):8279-8284.
14. Chao C, Klein NP, Velicer CM, et al. Surveillance of autoimmune conditions following routine use of quadrivalent human papillomavirus vaccine. J Intern Med. 2012;271(2):193-203.
15. Klein NP, Hansen J, Chao C, et al. Safety of quadrivalent human papillomavirus vaccine administered routinely to females. Arch Pediatr Adolesc Med. 2012;166(12):1140-1148.
16. Markowitz LE, Dunne EF, Saraiya M, et al; CDC. Human papillomavirus vaccination: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. 2014;63(RR-05):1-30.
17. Drolet M, Bénard É, Boily MC, et al. Population-level impact and herd effects following human papillomavirus vaccination programmes: a systematic review and metaanalysis. Lancet Infect Dis. 2015;15(5):565-580.
18. Romanowski B. Long term protection against cervical infection with the human papillomavirus: review of currently available vaccines. Hum Vaccine. 2011;7(2):161-169.
19. Petrosky E, Bocchini JA Jr, Hariri S, et al; CDC. Use of 9-valent human papillomavirus (HPV) vaccine: updated HPV vaccination recommendations of the Advisory Committee on Immunization Practices. MMWR. 2015;64(11):300-304.
20. Joura EA, Giuliano AR, Iversen OE, et al. A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. N Engl J Med. 2015;372(8):711-723.
21. Luxembourg A, Bautista O, Moell er E, et al. Design of a large outcome trial for a multivalent human papillomavirus L1 virus-like particle vaccine. Contemp Clin Trials. 2015;42:18-25.
22. Markowitz L. CDC Expert Commentary. Common Questions About 9-Valent HPV Vaccine. Medscape Pharmacists. June 22, 2015.
23. Advisory Committee on Immunization Practices (ACIP). Recommended Immunization Schedules for Persons Aged 0 Through 18 Years. United States. 2016.
24. CDC. Human papillomavirus vaccination coverage among adolescent girls, 2007-2012, and postlicensure vaccine safety monitoring, 2006-2013—United States. MMWR. 2013; 62(29):591-595.
25. CDC. National, Regional, State, and Selected Local Area Vaccination Coverage Among Adolescents Aged 13–17 Years — United States, 2014. MMWR. 2015;64(29):784- 792.26. CDC.
26. Human Papillomavirus (HPV). For Clinicians. HPV: You Are the Key to Cancer Prevention. Page last updated September 30, 2015.
27. CDC. Human Papillomavirus Vaccination Coverage Among Adolescents, 2007–2013, and Postlicensure Vaccine Safety Monitoring, 2006–2014 — United States. MMWR. 2014;63(29):620-624.
28. Newitt VN. HPV vaccination: Are you doing enough to make sure that your patients are protected? Nurse Pract Perspect. 2015;2(4):32-36.
29. Chao C, Preciado M, Slezak J, Xu L. A randomized intervention of reminder letter for human papillomavirus vaccine series completion. J Adolesc Health. 2015;56(1):85-90.
30. Bar-Shain DS, Stager MM, Runkie AP, et al. Direct messaging to parents/guardians to improve adolescent immunizations. J Adolesc Health. 2015;56(5 suppl):S21-S26.