
SW, a 42-year-old female, presented to the women’s health clinic for vaginal burning, an increase in vaginal discharge, and dyspareunia for 3 weeks. SW lives with her partner and has been in a monogamous heterosexual relationship for the past 4 years. Over the last 3 weeks, her vaginal burning increased from mild discomfort rated 2/10 to moderate/severe irritation rated 6–7/10. This has prevented SW from engaging in sexual intercourse due to vaginal pain. She reports fear that her ongoing avoidance of sexual intercourse will cause dissatisfaction in her relationship. SW tells the nurse practitioner (NP) she has had several bacterial vaginosis (BV) infections over the past 3 years and was seen at another clinic and treated for BV with metronidazole a month ago. On questioning about her symptoms at that time, SW notes that they were a bit different in that she had some slight burning in the vagina and that the metronidazole had not provided relief. It is since that time that the burning and discharge has increased.
Due to her history of recurrent BV, SW has attempted to self-treat by using nightly boric acid vaginal suppositories for the past 7 days with no symptom relief. Per her mother’s advice, SW has taken a daily probiotic and changed her diet to include whole Greek yogurt and kimchi to boost the health of her vaginal microbiome. SW wears white cotton underwear and washes undergarments separately from her other laundry with a dye-free and fragrance-free detergent. She showers with warm water, does not use soap on her genitals, and does not douche.
SW has a medical history significant for interstitial cystitis that is diet controlled and denies any current dysuria, hematuria, or urinary frequency. She reports that she has had 2 to 3 BV infections every year for the last 3 years. Historically, BV symptoms have resolved with metronidazole. SW had a spontaneous miscarriage 1 year ago. She had been on combination oral contraceptives since that time but discontinued these 2 weeks ago because she wanted to see if being off hormones would help her symptoms improve. SW reports her last period was 2 weeks ago, and she has not had sexual intercourse since.
An examination reveals no inflammation or lesions on the external genitalia, no vulvar tenderness, and no inguinal lymphadenopathy. The vaginal walls and cervix are erythematous with scattered petechiae. A copious amount of yellow discharge without malodor is noted. There is no cervical motion tenderness. Prior to any diagnostic testing, the NP considers that SW’s symptoms and examination findings could indicate vaginal candidiasis or trichomoniasis and that chlamydia or gonorrhea should be ruled out because of the vaginal discharge and cervical erythema. Bacterial vaginosis does not seem likely because it is not an inflammatory infection, discharge is often malodorous, and symptoms of vaginal burning and dyspareunia are not expected. Also, a whiff test was negative for an amine odor. Given the unlikelihood of BV, the NP is surprised at finding a vaginal pH greater than 4.5. What could this indicate? An alkaline vaginal pH is noted with BV and also with vaginal atrophy as might be seen with estrogen deprivation. SW is 42 years old, has regular periods, and an exam showed rugated vaginal walls, so a diagnosis of vaginal atrophy is excluded. Wet mount microscopy (WMM) of vaginal discharge provides revealing findings. There are few lactobacilli, no pseudohyphae or yeast buds, no trichomonads, and no clue cells. Parabasal cells (cells that are smaller and rounder than squamous epithelial cells and have larger nuclei with small amount of cytoplasm) are seen and an increase in inflammatory cells noted as a leukocyte-to-epithelial ratio of greater than 1:1. The patient’s symptoms, physical examination findings, and WMM findings are indicative of a diagnosis of desquamative inflammatory vaginitis (DIV). The diagnosis was further confirmed by negative vaginal swab tests for BV, candidiasis, chlamydia, and gonorrhea.
Desquamative inflammatory vaginitis overview
Desquamative inflammatory vaginitis is a rare presentation of chronic vaginitis caused by a dysbiosis of the vaginal microbiome and occurs most commonly in perimenopausal women. Vaginal dysbiosis leads to a decrease in protective lactobacilli, which alters the normal balance of vaginal flora. BV, a polymicrobial disorder, is the most common vaginal dysbiotic condition. With DIV, there is a dysbiotic aerobic environment dominated by Escherichia coli, Staphylococcus aureus, group B streptococcus, or Enterococcus faecalis.1 The dysbiotic vaginal microbiome of DIV leads to immune-mediated vaginal inflammation targeted on the vaginal mucosa and results in persistent nonodorous, purulent discharge that causes ongoing discomfort and irritation.2
The exact etiology of the vaginal dysbiosis is unknown. The vaginal microbiome in reproductive-age women is a complex balance of pH, lactobacilli, and hormonal levels dominated by estrogen, with transient fluctuations dependent on sexual activity, menses, and personal hygiene practices.3 Even slight changes to the microbiota of the vagina can interrupt the vaginal barrier and disrupt the balance of the vaginal microbiome. Increase in vaginal pH and changes to the vaginal epithelial barrier are risk factors to developing DIV.3 Bacterial infection, vitamin D deficiency, and estrogen deficiency have been disproved for development of DIV.2
Present research suggests that DIV might have systemic inflammatory roots that interrupt the vaginal flora and cause chronic irritation.3 It is associated with increased risk of STI acquisition, chorioamnionitis, preterm labor, and pelvic inflammatory disease.4
DIV is a noncommunicable inflammatory process and is a diagnosis of exclusion. It can be challenging to diagnose because of lack of healthcare provider awareness, similarities in clinical presentation to other causes of vaginitis, and lack of definitive tests. As healthcare provider knowledge and appropriate diagnosis of DIV are low, accurate reporting of incidence and prevalence are lacking, although these are believed to range from 0.8% to 4.3%.2
Diagnosis and treatment
Diagnosis of DIV is indicated by vaginal inflammation marked by spotted ecchymosis or petechiae, erythema, focal or linear erosions, and at least one of these patient-reported symptoms: vaginal discharge, dyspareunia, pruritus, burning, and irritation; a pH greater than 4.5; microscopy of vaginal flora containing an increased number of parabasal and inflammatory cells and a leukocyte-to-epithelial ratio greater than 1:1; and exclusion of BV, trichomoniasis, and candidiasis (Table 1).1 Gonorrhea, chlamydia, atrophic vaginitis, and use of vaginal irritants should also be excluded.
Table 1. Diagnosis of desquamative inflammatory vaginitis1-2,7-8</sup
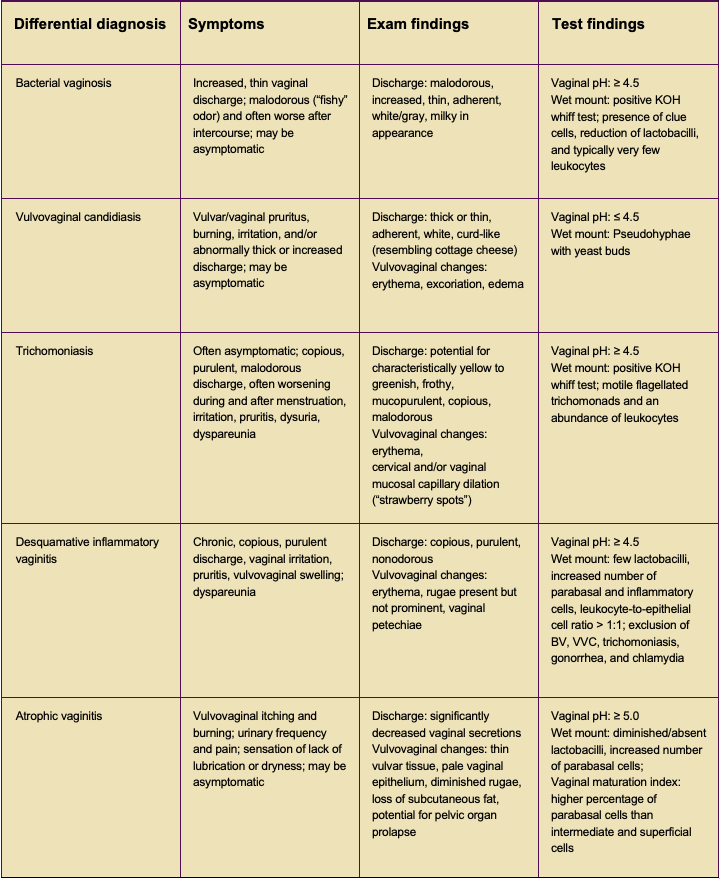
BV, bacterial vaginosis; KOH, potassium hydroxide; VVC, vulvovaginal candidiasis.
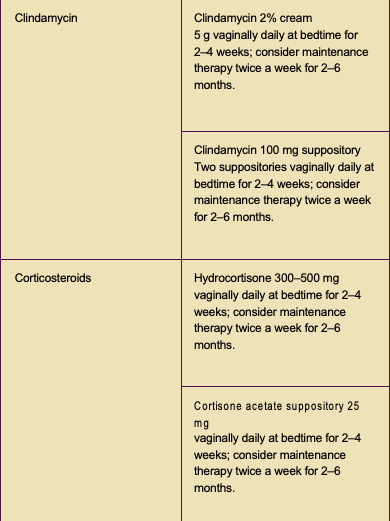
Clindamycin and hydrocortisone are the recommended treatments for DIV. Because DIV can recur, maintenance therapy may be indicated (Table 2).5 Data on the use of clindamycin in all trimesters of pregnancy and during breastfeeding are reassuringly safe.
SW was treated with a 2-week course of nightly 2% vaginal clindamycin cream and nightly vaginal hydrocortisone cream 500 mg. She was encouraged to continue her already established vaginal hygiene practices and advised to return if symptoms recur. She restarted her combination oral contraceptives. Symptoms resolved with treatment, and the patient was not seen again in the clinic until her next annual exam.
Table 2. Treatment of desquamative inflammatory vaginitis5
Conclusion
Desquamative inflammatory vaginitis falls under the umbrella of chronic vaginitis. Chronic vaginitis is characterized by prolonged and recurrent inflammation or infection of the vagina. The term is not a true diagnosis but rather an array of symptoms encompassing vulvovaginal itching, burning, irritation, dyspareunia, and abnormal vaginal odor or discharge. Chronic vaginal symptoms are a frequent reason for women to visit their healthcare provider. When an accurate diagnosis is not made and appropriate treatment is not initiated in a timely manner, additional sequelae such as chronic pain, discomfort with self or others, periods of absence from school or work, and withdrawal from social spheres can occur.6
DIV is not a common cause of inflammatory vaginal symptoms. When patients present with symptoms of vaginitis, it is appropriate for the workup to include common etiologies such as candidiasis, trichomoniasis, chlamydia, gonorrhea, and vaginal atrophy. However, when these diagnoses are excluded or for patients presenting with recurrent or persistent symptoms of vaginal discharge, pruritus, burning, irritation, and dyspareunia who have not responded to treatment, providers should be cognizant of other less common causes including DIV. Early diagnosis and treatment can significantly improve patients’ overall quality of life by decreasing pain and improving sexual health.
Leila M. Aruri is a registered nurse, student-nurse midwife and family nurse practitioner, and MSN candidate at Vanderbilt University School of Nursing in Nashville, Tennessee. Sarena Lesem is a registered nurse, IBCLC, student-nurse midwife, and MSN candidate at Vanderbilt University School of Nursing. Jessica N. Wellette is Assistant Professor of Nursing at Vanderbilt University School of Nursing and WHNP at VUSN Faculty Nurse-Midwife and Primary Care Practice in Nashville, Tennessee. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(6):34-37. doi: 10.51256/ WHC122334
References
1 Marnach ML, Wygant JN, Casey PM. Evaluation and management of vaginitis. Mayo Clin Proc. 2022;97(2):347-358.
2 Martin CD, Holland AC. Desquamative inflammatory vaginitis: a closer look. J Nurse Pract. 2020;16(10):732-734.
3 Paavonen J, Brunham RC. Bacterial vaginosis and desquamative inflammatory vaginitis. N Engl J Med. 2018;379(23):2246-2254.
4 Brunham RC, Paavonen J. Reproductive system infections in women: lower genital tract syndromes. Pathog Dis. 2020;78(5):ftaa022.
5 Borella F, Grincevičienė Š, Preti M, et al. Aerobic vaginitis/desquamative inflammatory vaginitis. In: Vieira-Baptista P, Stockdale CK, Sobel J, eds. International Society for the Study of Vulvovaginal Disease. Recommendations for the Diagnosis and Treatment of Vaginitis. Lisbon, Portugal: Admedic; 2023:149-150. doi:10.59153/adm.rdtv.001.
6 Paavonen JA, Brunham RC. Vaginitis in nonpregnant patients. ACOG Practice Bulletin no. 215. Obstet Gynecol. 2020;135(5):1229-1230.
7 Schuiling KD, Likis FE. Gynecologic Health Care. With an Introduction to Prenatal and Postpartum Care. 4th ed. Jones & Bartlett Learning; 2020.
8 Abdallah M, Augenbraun MH, McCormack W. Vulvovaginitis and cervicitis. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 9th ed. Philadelphia, PA: Elsevier; 2020:1462-1476.