
Eating disorders are associated primarily with adolescents and young adults. Women are most at risk for eating disorders in these populations. Women of all ages, however, may exhibit potentially detrimental eating behaviors. Evidence indicates that middle-aged and older women may have disordered eating patterns. Therefore, all women should be screened at a primary care women’s health visit to raise awareness of the topic and to intervene to prevent health complications.
If one were to associate words to describe the person with disordered eating, the typical first thoughts are young, female, overachiever, and altered body image. Rarely would anyone, even healthcare providers, associate the words mature, middle aged, or older with disordered eating issues or a diagnosis. Yet, do all with disordered eating present as adolescents or young adults? What happens to women who were diagnosed in their teens or early 20s as they age? Does the problem resolve, particularly if treatment was sought; does it become suppressed; or does it resurface as the person struggles through difficulties that may manifest at various times such as childbearing, loss and grief, changes in relationships, and employment in their lifetime? This article addresses disordered eating prevalence, associated factors, and potential complications in midlife and older women. Guidance is provided on identifying disordered eating in these age groups.
Eating disorder classifications and complications
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) describes five main categories of feeding and eating disorders1:
• Anorexia nervosa: Restriction of energy intake leading to a significantly low body weight; intense fear of gaining weight or becoming fat; and disturbance in the way in which one’s body weight or shape is experienced.
• Bulimia nervosa: Recurrent episodes of binge eating (discrete amount of time, lack of control); recurrent inappropriate compensatory behavior not to gain weight (eg, self-induced vomiting, misuse of laxatives, diuretics, medications, exercising); both behaviors occurring at least once weekly for 3 months; self-evaluation unduly influenced by body shape and weight; and disturbance not occurring exclusively during episodes of anorexia nervosa.
• Binge eating disorder: Definition of binge eating as in bulimia nervosa associated with three (or more) of the following: eating much more rapidly than normal; eating until feeling uncomfortably full; eating large amounts of food when not feeling physically hungry; eating alone because of feeling embarrassed by how much one is eating; and feeling disgusted with oneself, depressed, or very guilty afterward. Binge eating is associated with compensatory behavior and occurs on average at least once weekly for 3 months.
• Other specified feeding or eating disorder: Symptoms characteristic of a feeding or eating disorder causing clinically significant distress or impairment in social, occupational, or other important areas of functioning predominate but do not meet full criteria.
• Unspecified feeding or eating disorders: Same as above, but used in situations in which the clinician chooses not to specify the reason criteria are not met and includes presentations in which there is insufficient information.1
Recently in the literature, variations on the theme of disordered eating have been described. The idiomatic terms of drunkorexia and diabulimia, not recognized by the DSM-5, have arisen. The former refers to calorie restriction prior to ingestion or in anticipation of ingestion of alcohol, plus excessive exercise as a possible third component.2 The motivation may be to not gain weight or get drunk faster.3 The latter refers to restricting insulin by persons with diabetes to lose weight.4
Health complications abound with prolonged disordered eating behaviors and become riskier as the person ages. Comorbidities may include cardiovascular disease, gastrointestinal disorders, kidney problems, metabolic issues, endocrine shifts, osteoporosis, and arthritis.5–7 Particularly in older persons with anorexia nervosa, loss of bone density may lead to decreased mobility and a higher fracture rate.5 Bulimia nervosa is associated with cardiopulmonary problems, electrolyte imbalance, gastroesophageal reflux, constipation, diarrhea, oral health problems, muscle weakness, and gynecologic disorders.7
In a longitudinal Canadian study of 818 women hospitalized with bulimia nervosa, researchers found it associated with ischemic heart disease, atherosclerosis, and cardiac conduction as well as 21.93 times the risk of myocardial infarction at 2-year follow-up and 14.13 times the risk at 5-year follow-up.8 Patients with bulimia nervosa had a 4.72 times the risk of death than the comparison group of women hospitalized for pregnancy-related events up to 8 years post hospitalization.8
The most common altered eating pattern as a person ages is binge eating disorder.9 Obesity and its sequelae are directly related to complications and possibly even death from binge eating disorder.7 Metabolic syndrome, insulin resistance, type 2 diabetes mellitus, and dyslipidemia all raise the person’s risk for health issues, particularly after age 40 years. Identification of persons with binge eating disorder is a challenge for clinicians. If the person’s reported attempts to lose weight have failed despite lifestyle changes, however, specific eating behaviors need to be investigated and a referral to a nutrition consultant may be appropriate.
Current knowledge about eating disorders in midlife and older women
Although research on eating disorders in midlife and older women is limited, studies reported in the past 10 years provide some insights. A decade ago, it was noted that 67% of women older than age 30 years were dissatisfied with their body weight.10 In 2018, researchers also noted that body image dissatisfaction may be one of the factors affecting eating patterns in older women to the same degree as in younger populations.5 This is not to say that body weight and body image dissatisfaction cause eating disorders across the lifespan, but the psychological predictor of body dissatisfaction remains fairly stable throughout life.5 Contributing factors to body dissatisfaction as a person ages include body weight increase, especially after pregnancy, and age-related musculoskeletal and hormonal changes that alter body shape. Women particularly may be trying to stave off aging and in their search for a youthful appearance turn to weight loss as an imperative. The term “perimenopausal eating disorder” was coined by authors theorizing that hormonal influences play a role in developing eating disorders.11
In the United Kingdom in 2010, researchers interviewed a small sample of patients older than age 50 years who presented to a national eating disorder center. Their aim was to determine whether the eating disorder was of new onset or of a chronic nature. They found no evidence of late-onset disorders and that the psychiatric issues were lifelong.12 Other investigators tended to agree with this finding a few years later, stating that it seems anorexia in middle-aged and elderly women is primarily a chronic emergence of an earlier-onset problem.6
In one study, researchers examined first inpatient admissions assessment records for disordered eating between 1989 and 2006 and then in a separate study from January through May 2007. They compared middle-aged women with younger women seeking treatment. The self-reported onset was 17.0 years for those age 18 to 39 years and 21.4 years for those age 40 years and older.13 Although treatment was sought at an older age, the onset was still in the young adult range.
Prevalence
In 2010, investigators reported a 1% prevalence of women presenting for eating disorder treatment at age 50 years and older.12 Other researchers, however, found a significant increase of admission for treatment in women age 40 years and older, from an average of 4.7% in 1989 to 2001 to 11.6% in 2002 to 2006.13 In a 2006 study, it was reported that of 175 participants (women age 60-70 years), 3.8% met the criteria for an eating disorder.14 More recently, in 2018, it was found that in a sample of 245 women age 60 to 90 years, 11.84% had clinical levels of disordered eating according to results on the Eating Attitudes Test-26.5
The results of these studies are not associated with normal variations in eating patterns as a person ages and need to be differentiated. As a person ages, generally appetite decreases as well as caloric intake due to reduced energy expenditure, decreased gastric motility, and lessened taste and smell response. The latter physical changes may be termed “anorexia of aging” and are considered a normal consequence affecting 16% to 20% of persons older than age 65 years.6,15
These findings from research studies do highlight that eating disorders occur in midlife and beyond, no matter if the disordered eating pattern may be of new onset. The numbers of midlife and older women with disordered eating may be underestimated due in part to older adults’ embarrassment at having a disorder associated with “teenage pathology.”7 According to results from a 2017 study, 3.5% of older women (> age 40 years) met the DSM-5 criteria for an eating disorder.16
Associated factors
Factors associated with disordered eating in older women are similar to those seen in their younger counterparts.5 Psychological symptoms may be the chief complaint of the history of the present illness. Similar to critical periods in adolescents and young adults, transitions during menopause make older women more vulnerable to associated changes in appearance and concerns of aging.16 In one study of elderly women (age 60–90 years), sociocultural pressures to be thin and attain perfection as well as the onset of depression were significantly related to eating pathology.5 In a descriptive study of patients age 50 to 68 years (only 1 male) who presented to a national eating disorder center, psychiatric comorbidity was revealed: depression (46%), anxiety disorders (31%), alcohol dependency syndrome (19%), and personality disorder (19%).12
Weight suppression, defined as the difference between highest past nonpregnancy weight and current weight (current weight < highest weight), and weight elevation (current weight > lowest weight) were associated with eating disorder symptomatology in women age 50 years and older.17 In the Gender and Body Image study, 1,776 female participants completed online demographic and eating psychopathology questions. Women who had higher scores on weight suppression and weight elevation questions were more likely to engage in current weight loss attempts, extreme lifetime restriction, and skipping meals over lifetime. Those with higher weight suppression scores reported more binge eating, greater frequency of weight checking, overvaluation of shape and weight, and lifetime fasting. Those scoring higher on weight elevation questions reported negative impacts of eating and dieting.17
In one review of studies published between 1930 and 2013 that evaluated eating disorders in older adults, it was noted that late-life eating disorders were associated with anxiety and depression but less substance abuse, self-harming behaviors, and suicide attempts.7 The authors of the review did not specifically define late life. They did acknowledge, however, that an onset after the age of 40 years is generally considered late onset. The studies related to both late-onset disordered eating as well as those having been diagnosed in the traditional age group (16–25 years) but who are now in midlife or older age.7
Identifying eating disorders in midlife and older women
It appears likely from the minimal research on the topic that most midlife and older women presenting with disordered eating developed behaviors earlier in their lives. Perhaps they were diagnosed, but as a person’s healthcare provider changes and without interoperable electronic health records, unless the person self-reports, that data may remain hidden. Women with eating disorders such as anorexia nervosa, bulimia nervosa, binge eating, and other related diagnoses do not generally present as emaciated, hypokalemic, dehydrated, and amenorrheic. The person may not choose to reveal their weight loss strategies and/or coping and eating behaviors unless directly asked. Awareness and recognition of the probable signs are key for the clinician to provide holistic care. Researchers recommend screening women with a history of bulimia nervosa for cardiovascular disease for prevention and treatment, which emphasizes the importance of obtaining a thorough health history as the person ages.8 Trust gained by the clinician is a key element in eliciting long-term accurate health histories with possible influential health factors.
Simple questions during the health history and/or physical exam may be posed to the midlife or older woman to open the door to discussion. “Do you consider yourself a healthy person?” may open the dialogue. Follow-up, more direct questions may be, “Do you ever restrict your food intake?” or “Do you ever make yourself vomit or use laxatives to control your weight?” to bring up the topic of eating habits. If a concern is raised, a dietary recall for the day may provide insight. These are simple questions sometimes without simple answers.
These questions may be used to start the conversation in a face-to-face interview, although the elicited information would not give any historical background about disordered eating behaviors. Issues arise with self-report when collecting data, so it is difficult to say with certainty as to whether age of onset indicates onset of behaviors or actual diagnosis in each case. For women older than their mid-20s, however, most likely the eating disorder behaviors developed over years were exacerbated with life-changing stressful events such as pregnancy, childbirth, and divorce. Age at which treatment was sought may be many years after onset.
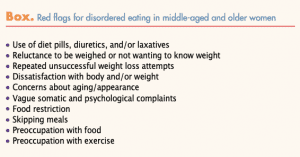
The use of one of the formal screening measures that are available may be considered when red flags are raised or the answers to questions are concerning (Box). Several formal screening measures are available. The Eating Disorder Examination Questionnaire 8 (EDE-Q-8) adapted from the longer Eating Disorder Examination Questionnaire (EDE-Q) with eight questions is manageable in the clinical setting to ascertain an initial global assessment and has good psychometric properties.18 Questions address: restraint over eating; food avoidance; preoccupation with food; feelings of fatness; desire to lose weight; guilt about eating; dissatisfaction with weight; and discomfort with seeing one’s body.
Other screening tools include the Screen for Disordered Eating (SDE), Eating Disorder Screen for Primary Care (EDS-PC), and SCOFF (sick, control, one, fat, food) screener.19 The SDE screen incorporates questions from the longer SCOFF instrument that was developed with DSM-4 categories. The SDE is considered valid in primary care due to its versatility in identifying binge eating disorder. The SDE is limited in that it is a self-report measure and therefore may have inherent bias. The SDE is not age specific. The SDE questions are as follows:
• Do you often feel the desire to eat when you are emotionally upset or stressed?
• Do you often feel that you can’t control what or how much you eat?
• Do you sometimes make yourself throw up (vomit) to control your weight?
• Are you often preoccupied with a desire to be thinner?
• Do you believe yourself to be fat when others say you are thin?
A 2003 study compared the SCOFF and the EDS-PC, a 5-question measure.20 Analysis indicated that although the screens were not much different, the SCOFF was less sensitive than the EDS-PC and the EDS-PC questions were more likely to rule out an eating disorder.20 The questions from the EDS-PC most likely to rule out an eating disorder are:
• Does your weight affect the way you feel about yourself?
• Are you satisfied with your eating patterns?20
The EDS-PC questions most likely to rule in an eating disorder are:
• Do you worry that you have lost control over how much you eat?
• Do you make yourself sick when you are uncomfortably full?
• Do you currently suffer with or have you ever suffered in the past with an eating disorder?
• Do you ever eat in secret?20
In a 2019 opinion, based on previous evidence from 2008 and 2010, the authors deemed the SCOFF questionnaire and the EDE-Q as useful primary care screening instruments for eating disorders.21 A recent meta-analysis and review of 25 validation studies of the SCOFF, however, found that although the tool is useful for younger women, there is not enough evidence to support its use in primary care and community-based settings. It also does not cover the eating disorder categories in DSM-5.22
Yet perhaps the most important question to ask the midlife or older woman is whether or not she has a past history of an eating disorder. The answer to this question will guide the discussion between the clinician and client.
If the person is not ready or reluctant to identify or denies there is a problem, the National Eating Disorders Association has an online screening measure for those age 13 years and older that may help women recognize they are at risk.23 Mental Health America and the Healthy Minds Network have also identified many thousands at risk through online screening tools for the layperson.23
Conclusion
If midlife and older women with underlying eating disorders have comorbidities with their younger counterparts, is it not feasible that some of the behaviors may carry over to adulthood or begin to be exhibited at a later age? No matter what the age group, identification of eating disorders in the primary care setting can present a challenge for the clinician especially in the early phases prior to physical changes and reduction in the quality of life.24
The wise clinician listens for cues. Astute history-taking skills with sensitivity to disordered eating issues are necessary to elicit potentially detrimental behaviors. A trusting relationship between clinician and patients is necessary to assist in managing interventions. The clinician needs to develop a strategy with the patient as to how to handle the problem. Referral sources should be made available to the person when an eating disorder is identified such as counseling, nutrition, and social work if assistance is needed to cover costs of services. An interdisciplinary interventional approach is best. Identification and treatment and increasing treatment coverage may decrease eating disorder-related morbidity and mortality.25 =
Jo Ann L. Nicoteri is Assistant Professor and a family nurse practitioner in the Department of Nursing/Student Health Services at the University of Scranton in Scranton, Pennsylvania. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
- Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Washington DC: American Psychiatric Association; 2013.
- Wilkerson AH, Hackman CL, Rush SE, et al. “Drunkorexia”: understanding eating and physical activity behaviors of weight conscious drinkers in a sample of college students. J Am Coll Health. 2017;65(7):492-501.
- Roosen KM, Mills JS. Exploring the motives and mental health correlates of intentional food restriction prior to alcohol use in university students. J Health Psychol. 2015;20(6):875-886.
- Davenport L. Emotional support key to unlocking eating disorders in T2D. March 15, 2019. https://www.medscape.com/viewarticle/910463.
- Midlarsky E, Marotta AK, Pirutinsky S, et al. Psychological predictors of eating pathology in older adult women. J Women Aging. 2018;30(2):145-157.
- Podfigurna-Stopa A, Czyzyk A, Katulski K, et al. Eating disorders in older women. Maturitas. 2015;82(2):146-152.
- Luca A, Luca M, Calandra C. Eating disorders in late-life. Aging Dis. 2014;6(1):48-55.
- Tith RM, Paradis G, Potter BJ, et al. Association of bulimia nervosa with long-term risk of cardiovascular disease and mortality among women. JAMA Psychiatry. 2020;77(1):44-51.
- Smink FRE, van Hoeken D, Hoek HW. Epidemiology of eating disorders: incidence, prevalence and mortality rates. Curr Psychiatry Rep. 2012;14(4):406-414.
- Carr M, Kaplan C. Midlife women with anorexia nervosa: a review of the literature. Am J Nurse Practitioners. 2010;14(6):8-14.
- Baker JH, Runfola CD. Eating disorders in midlife women: a perimenopausal eating disorder? Maturitas. 2016;85:112-116.
- Scholtz S, Hill LS, Lacey H. Eating disorders in older women: does late onset anorexia nervosa exist? Int J Eat Disord. 2010;43(5):393-397.
- Ackard DM, Richter S, Frisch MJ, et al. Eating disorder treatment among women forty and older: increases in prevalence over time and comparisons to young adult patients. J Psychosom Res. 2013;74(2):175-178.
- Mangweth-Matzek B, Rupp CI, Hausmann A, et al. Never too old for eating disorders or body dissatisfaction: a community study of elderly women. Int J Eat Disord. 2006;39(7):583-586.
- Dell’Aquila G, Landi F, Euschi P, et al. Prevalence and potentially reversible factors associated with anorexia among older nursing homes residents: results from the ULISSE project. Eur Geriatr Med. 2013;4(suppl 1):S45.
- Mangweth-Matzek B, Hoek HW. Epidemiology and treatment of eating disorders in men and women of middle and older age. Curr Opin Psychiatry. 2017;30(6):446-451.
- Goodman EL, Baker JH, Peat CM, et al. Weight suppression and weight elevation are associated with eating disorder symptomatology in women age 50 and older: results of the gender and body image study. Int J Eat Disord. 2018;51(8):835-841.
- Kliem S, Möβle T, Zenger M, et al. The Eating Disorder Examination – Questionnaire 8: a brief measure of eating disorder psychopathology (EDE-Q8). Int J Eat Disord. 2016;49(6):613-616.
- Maguen S, Hebenstreit C, Yongmei L, et al. Screen for disordered eating: improving the accuracy of eating disorder screening in primary care. Gen Hosp Psychiatry. 2018;50(1):20-25.
- Cotton MA, Ball C, Robinson P. Four simple questions can help screen for eating disorders. J Gen Intern Med. 2003;18(1):53-56.
- Seferovic A, Dianes GN, Juan B, et al. What is the best screening tool for eating disorders in the primary care setting? Evidence-Based Practice. 2019;22(3):12.
- Kutz AM, Marsh AG, Gunderson CG, et al. Eating disorder screening: a systematic review and meta-analysis of diagnostic test characteristics of the SCOFF. J Gen Intern Med. 2019; November 8. [Online ahead of print]
- Taylor CB, Graham AK, Fitzsimmons-Craft EE, et al. Optimizing eating disorder treatment outcomes for individuals identified via screening: an idea worth researching. Int J Eat Disord. 2019;52(11):1224-1228.
- Sim LA, McAlpine DE, Grothe KB, et al. Identification and treatment of eating disorders in the primary care setting. Mayo Clin Proc. 2010;85(8):746-751.
- Ward ZJ, Rodriguez P, Wright DR, et al. Estimation of eating disorders prevalence by age and associations with mortality in a simulated nationally representative US cohort. JAMA Netw Open. 2019;2(10):e1912925.