
Gestational diabetes mellitus (GDM) is a common condition affecting approximately 2% to 10% of all pregnancies in the United States.1 Incidence and prevalence of GDM are increasing because of poor-quality diet, low levels of physical activity, obesity or overweight, and older maternal age.2 Hyperglycemia due to endocrine metabolic dysfunction typifies GDM, when diagnosed in the second or third trimester of pregnancy.3 During pregnancy, the fetus and the placenta produce hormones that increase insulin resistance. GDM occurs when a pregnant person’s body cannot produce enough extra insulin to meet the demands resulting in elevated blood glucose levels.4 The dysfunction of beta cells, which are responsible for insulin production and release in the pancreas, is a significant component of GDM pathophysiology and is intensified by insulin resistance.3 Beta cell dysfunction, although complex, results in the cells’ inability to compensate for pregnancy demands with increased production of insulin, thereby contributing to hyperglycemia. Hyperglycemia in pregnancy increases the risk of preeclampsia and fetal macrosomia, and predisposes the person to later development of type 2 diabetes mellitus and children to obesity.5
Lifestyle behaviors are the primary focus of preventive measures aimed to minimize the impact of GDM on a pregnant person and manage the effects of GDM on pregnancy.3 Treatment for GDM varies, but an initial recommendation is for the pregnant person to adjust their diet. Approximately 15% of individuals with GDM will require pharmacologic management with oral hypoglycemics or insulin to control their blood glucose, and consequently, both their own and their fetus’s metabolic needs.4 Glycemic targets in pregnancy are stricter than in nonpregnant individuals, making it important that individuals with GDM eat consistent amounts of carbohydrates and other nutrients to avoid hypoglycemia or hyperglycemia.6
Medical nutrition therapy (MNT) offers an individualized nutrition plan developed by a registered dietician (RD) or a registered dietician nutritionist (RDN) familiar with the management of GDM. This food plan should provide adequate calories to promote the health of the fetus and pregnant person, achieve glycemic goals, and promote adequate weight gain. An RD or RDN can be an invaluable asset to help people with GDM develop a diet around their specific needs or food preferences. An RDN certified in diabetes care and education (CDCES) offers advanced specialization in managing both diet and diabetes.
However, the availability of the expertise and guidance of RDs and RDNs can be inconsistent in resource-poor settings. When this is the case, and virtual visits are not feasible, midwives and women’s health nurse practitioners (WHNPs) can use appropriate resources and take the responsibility for comprehensive and holistic dietary education with consultation and referrals when needed. The purpose of this article is to provide midwives and WHNPs with current evidence-based guidelines surrounding nutrition and dietary education and sample meals to assist in counseling pregnant people with GDM.
Diet
Most nutrition recommendations center on a consistent distribution of carbohydrate intake.3,6,7 The Dietary Reference Intakes suggest a minimum of 175 g carbohydrates, a minimum of 71 g protein, and 28 g fiber, emphasizing monounsaturated and polyunsaturated fats while limiting intake of saturated and trans fats.6,8 There is no specific diet for GDM because every person is different relative to their dietary needs. However, there are some general guidelines for dietary modifications. Eating small meals throughout the day to spread out the amount of carbohydrates consumed is preferred.6 Increasing physical activity, like walking especially after meals, to help the body utilize carbohydrates more efficiently is recommended.9 Developing an awareness of portion size is essential. Portion size incorporates the notion that half of a meal plate should be non-starchy vegetables, a fourth of the plate lean protein, and the remaining fourth carbohydrates or starchy foods such as beans, legumes, fruit or dried fruit; vegetables such as potatoes, green beans, sweet potatoes, butternut or acorn squash, or pumpkin; and whole grain or whole grain products such as bread, pasta, or tortillas.10
Processed food usually has added sugar, salt, or fat, removing vital nutrients like fiber. Minimally processed foods such as whole wheat flour and fresh or frozen produce are healthier choices. Because blood glucose is already elevated, the pregnant person should avoid food or drinks with additional sugar. Foods that have not undergone any processing are known as whole foods and include fresh fruits, vegetables, whole grains, eggs, nuts, beans, and fish or shellfish. Thus, when providing education surrounding diet for individuals with GDM, the midwife or WHNP should emphasize lean proteins, whole grains, non-starchy vegetables, healthy fats, fruits, selected starchy foods, and healthy snacks.
Lean proteins
Lean protein is a source of protein that is low in saturated fat and consequently lower in calories. Lean proteins are preferred in pregnancy because they enable individuals to meet their protein intake requirements while promoting optimal heart health. Lean proteins also allow the body to use and absorb blood glucose more effectively, promoting a feeling of satiety after meals.11 See Box 1.
Box 1. Sources of lean protein
Chicken or turkey sausage, skinless
Eggs
Fish (eg, tilapia, tuna, cod, salmon, or
swordfish)
Low-fat dairy (eg, cheese, cottage cheese, low-fat or Greek yogurt, low-fat milk or
milk substitutes like almond, oat, or soy milk if not allergic)
Shellfish
Whole grains
Whole grains are ideal because they raise blood glucose less than refined grain products. To determine if a packaged food contains whole grain, the package ingredients list should include specific things like “whole wheat flour,” “whole oats,” or “buckwheat” within its first or second ingredients. Whole grain options include popcorn, oatmeal, brown rice, whole grain cereals, and whole wheat bread or pasta.
Nonstarchy vegetables
Nonstarchy vegetables are higher in fiber and lower in sugar and calories than starchy vegetables. They usually contain about 5 g carbohydrates per serving. Nonstarchy vegetables are high in essential nutrients like vitamins, minerals, and fiber. Intake of these vegetables is encouraged. Pregnant people can use nonstarchy vegetables as both a key component of a meal or for snacking to curb hunger. Nonstarchy vegetables are versatile and can be eaten raw, steamed, sauteed, baked without breading, grilled, or broiled. See Box 2.
Box 2. Nonstarchy vegetables
Broccoli
Carrots
Cauliflower
Celery
Cucumbers
Eggplant
Okra
Salad greens
Snow or sugar snap peas
Spaghetti squash
Spinach
Zucchini
Healthy fats
Healthy fats are monounsaturated and polyunsaturated fats that help the body absorb vitamins, provide energy, and protect the heart and brain from long-term disease. Healthy fats also help manage mood, promote mental clarity, fight fatigue, and promote adequate weight gain during pregnancy. Healthy fats promote proper brain and eye development in the fetus. Healthy fat options include nuts and nut butters, olive oil, avocado, and seeds.
Fruits
Eating whole fruit is encouraged during pregnancy. With GDM, however, fruit is encouraged in moderation because it contains fructose that can raise blood glucose levels. Eating too much fruit at one time can cause a sudden increase in blood glucose. Eating fruits with protein and fiber, however, can help keep blood glucose levels low and promote satiety. Individuals with GDM should avoid fruit juices that are high in sugar.
Starchy foods
Starchy foods affect blood glucose more than any other food. However, when eaten carefully and in moderation, starchy foods such as potatoes, rice, cereals, bread, and pasta provide energy and contain nutrients like calcium, iron, and B vitamins. Some starchy foods then are beneficial for individuals with GDM.
Smart snacking
The primary way to combat excessive weight gain and hunger during pregnancy is by eating small meals throughout the day. This includes breakfast, lunch, and dinner and two to four small snacks. See Box 3.
Box 3. Smart snacking examples
- Two tablespoons almond or peanut butter with one slice of whole wheat bread or an apple
- Small apple with 1 ounce cheddar cheese or low-fat mozzarella or Monterey Jack cheese
- Two to three cups plain, air-popped popcorn
- Five to six whole wheat crackers with 1 ounce cheddar cheese
- One cup plain low-fat or Greek yogurt with one cup mixed berries
- Half whole wheat pita or tortilla with one tablespoon hummus and carrot and cucumber slices
- Banana with nut butter (almond or peanut)
- Strawberries dipped in low fat or plain Greek yogurt
- Grapes and cheese cubes
- Roasted chickpeas
- Vegetable chips
Resources
Multiple resources exist online and in print to assist the midwife or WHNP in educating about and guiding dietary choices during pregnancy. Not all sources online are reliable, however, and many provide incomplete or incorrect information. Box 4 provides examples of reliable online resources. This author created a comprehensive cookbook replete with easy recipes to follow, including individuals with GDM, to ensure adequate caloric and nutrient intake occurs using fresh, healthy ingredients. A 3-day menu created using the author’s cookbook as a reference provides a sample the midwife or WHNP can use in the clinical setting (Table). It provides examples for meals and snacks as a foundation for further discussion and refinement based on individual needs and preferences. This sample menu and other reliable resources are intended to guide discussions between the midwife and WHNP and the person with GDM to develop a holistic, individualized meal plan that promotes nutrition and safety within a comprehensive treatment plan.12
Table. Sample 3-day menu for GDM
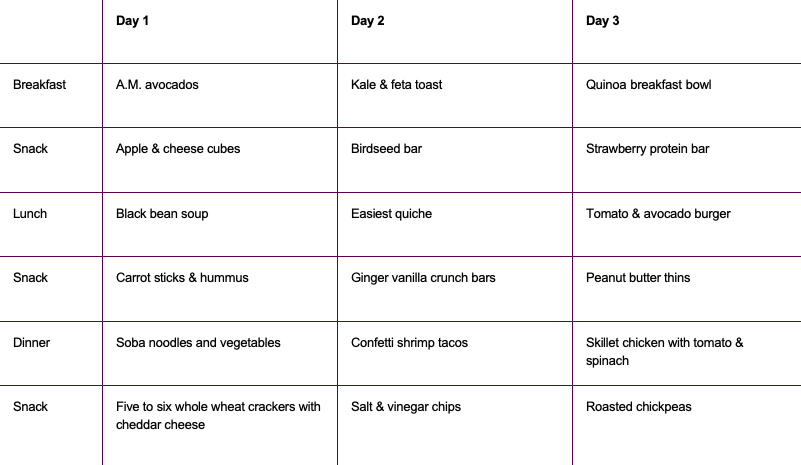
GDM, gestational diabetes mellitus.
Adapted from Quinn P. Prenatal Possibilities: Recipes for a Healthy PregnancyÉand Beyond.12 Used with permission.
Paul Quinn is on the emergency department staff at The Valley Hospital in Ridgewood, New Jersey. The author has no actual or potential conflicts of interest in relation to the contents of this article.
Box 4. Online resources
acog.org/womens-health/faqs/gestational-diabetesCenters for Disease Control and Prevention
cdc.gov/pregnancy/diabetes-gestational.htmlJohns-Hopkins Medicine
hopkinsmedicine.org/health/conditions-and-diseases/gestational-diabetes
March of Dimes
marchofdimes.org/find-support/blog/how-to-manage-gestational-diabetes
Mastering Diabetes
masteringdiabetes.org
National Institutes of Health of Diabetes and Digestive and Kidney Diseases
niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/gestational
Womens Healthcare. 2023;11(6):20-23. doi: 10.51256/ WHC122320
References
1 Gregory ECW, Ely DM. Trends and characteristics in gestational diabetes: United States, 2016-2020. Natl Vital Stat Rep. 2022;71(3):1-15.
2 Shah NS, Wang MC, Freaney PM. Trends in gestational diabetes at first live birth by race and ethnicity in the US. JAMA. 2021;326(7):660-669.
3 Helm MM, Izoura K, Basu A. Nutrition-education-based interventions in gestational diabetes: a scoping review of clinical trials. Int J Environ Res Public Health. 2022;19(19):12926.
4 Hess-Fischl A, Arevalo SJ. What to eat with gestational diabetes. Updated September 26, 2022. https://www.healthcentral.com/condition/gestational-diabetes/diet.
5 Mustafa ST, Hofer OJ, Harding JE, et al. Dietary recommendations for women with gestational diabetes mellitus: a systematic review of clinical practice guidelines. Nutr Rev. 2021;79(9):988-1021.
6 American Diabetes Association. 14. Management of diabetes in pregnancy: Standards of Medical Care in Diabetes–2021. Diabetes Care. 2021;44(suppl 1):S200-S210.
7 Egan AE, Dow ML, Vella A. A review of the pathophysiology and management of diabetes in pregnancy. Mayo Clin Proc. 2020;95(12):2734-2746.
8 Alexopoulos AS, Blair R, Peters AL. Management of preexisting diabetes in pregnancy: a review. JAMA. 2019;321(18):1811-1819.
9 Kapur K, Kapur A, Hod M. Nutrition management of gestational diabetes mellitus. Ann Nutr Metab. 2021;76(suppl 3):17-29.
10 Academy of Nutrition and Dietetics. Gestational diabetes nutrition therapy. NCM. 2023. https://www.nutritioncaremanual.org.
11 US Department of Agriculture. AskUSDA. What does “lean” and “extra lean” beef mean on a nutrition label? March 24, 2023. https://ask.usda.gov/s/article/What-does-lean-and-extra-lean-beef-mean-on-a-nutrition-label#:~:text=Lean%20means%20that%20100%20grams%20of%20beef%20%28about,fat%2C%20and%20less%20than%2095%20milligrams%20of%20cholesterol.
12 Quinn P. Prenatal Possibilities: Recipes for a Healthy Pregnancy…and Beyond. Olney, Maryland: Level Best Books; 2023.