
Menstruation is a part of life for individuals throughout the world. Many who menstruate have pain associated with their period (dysmenorrhea), heavy menstrual bleeding, and mood-related symptoms.1–4 Heavy menstrual bleeding can negatively alter daily lives and lead to anemia, making activities hard to complete.1,5 Dysmenorrhea is one of the most common menstrual symptoms, impacting up to 95% of women worldwide.6–8 Studies that have focused on young adults found menstrual symptoms can be disabling, causing discomfort, missed activities including work, and time spent looking for symptom relief and provider assistance.2,6,9,10 Research also suggests many individuals who menstruate have limited knowledge about menstrual symptoms and encounter stigma related to menstruation being known as a taboo topic.11,12 This cross-sectional, mixed methods study investigated how a sample of young adults age 18 to 25 years at a midwestern university experience menstruation, including impacts on various aspects of their life and perceived health. The purpose of this study was to understand how young adults perceive their quality of life in relation to their menstrual symptoms and how provider/patient relationships can impact symptom relief and health outcomes.
Methodology
Setting and sample
Recruitment was limited to those enrolled at a private liberal arts university in an urban metropolitan city in the midwestern United States. Inclusion criteria included individuals between the ages of 18 and 25 years and having experienced a menstrual cycle. Participants were recruited through university emails and fliers. There were 167 online survey participants and 16 focus group participants.
Data collection and analysis
The study started with an online survey (29–40 branched logic questions; consent included). The last question of the survey asked if participants were interested in participating in a virtual focus group. Incentives were provided. Ethical approval to conduct this study was obtained from the University’s Institutional Review Board. Survey questions were pilot-tested prior to use and related to menstrual symptoms such as bleeding, pain, and missed activities. Questions were adapted from two validated tools: the World Health Organization Quality of Life–BREF and the Impact of Female Chronic Pelvic Pain Questionnaire.13,14 These questionnaires were chosen specifically because they show a holistic and cross-cultural approach to quality of life and various impacts such as psychological, sexual, relationships, occupational, and emotional impacts on those with menstrual cycles.
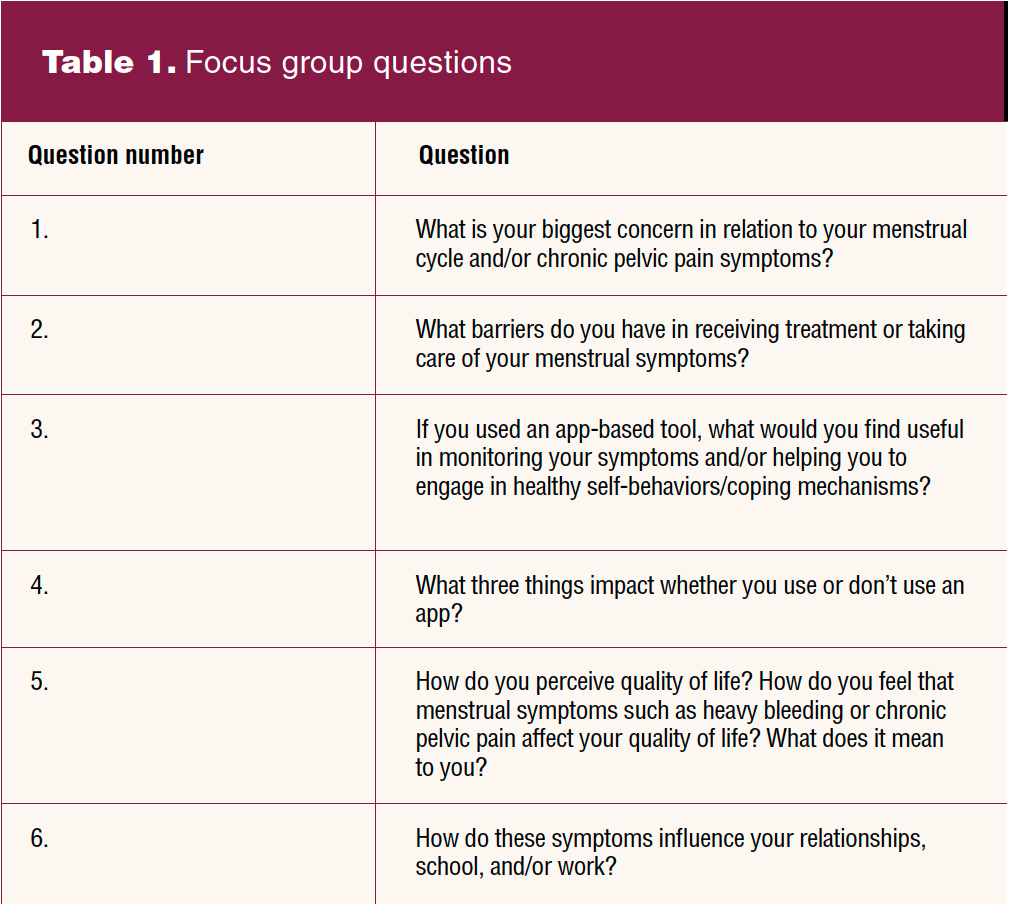
Three virtual focus groups with 18 participants total were facilitated by the study authors, and their sessions lasted approximately 60 minutes each. The audio was recorded. Data were stored on a password-protected computer and destroyed within 1 month. The six focus group questions expanded on what was asked in the survey to help gain further insight into how individuals reflect on their menstrual cycles, asking how individuals experience symptoms in relation to their quality of life, including barriers to treatment, use of tools to monitor symptoms/engage in self-care, and if any changes occur in daily activities and relationships. Focus group questions are listed in Table 1. Descriptive statistical analysis of the survey data was completed using Qualtrics software. Recordings of the focus groups were transcribed and analyzed using content analysis.
Results
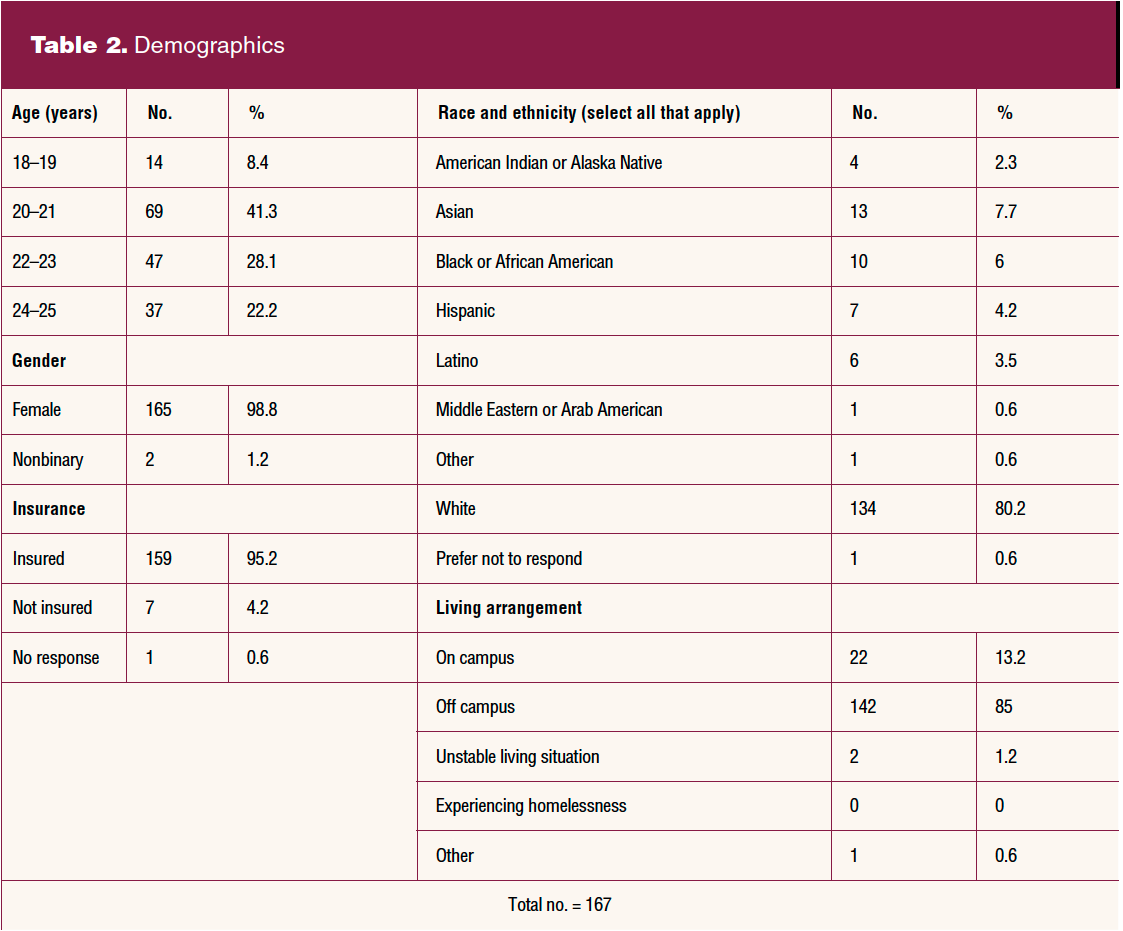
Demographic characteristics of participants are listed in Table 2. The age range of participants was 18 to 25 years, with the majority between the ages of 20 and 23 (69.4%). Nearly all reported their gender as female (1.2% nonbinary). The majority (80.2%) reported their race as White. A range of ethnicities was reported. Most participants had health insurance and lived off campus.
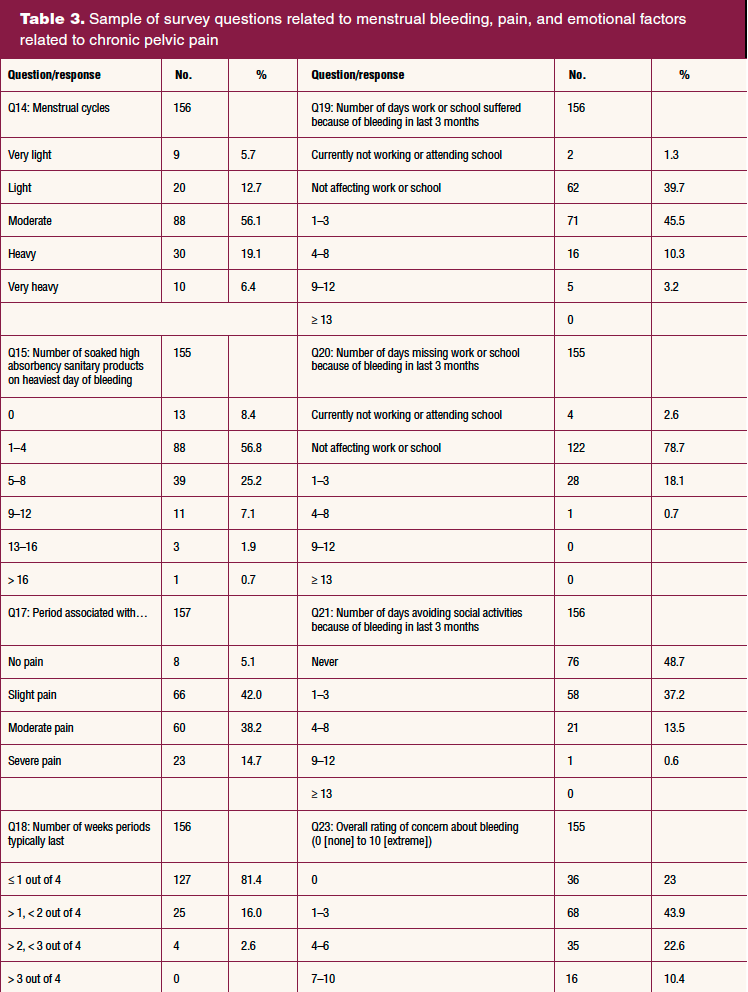
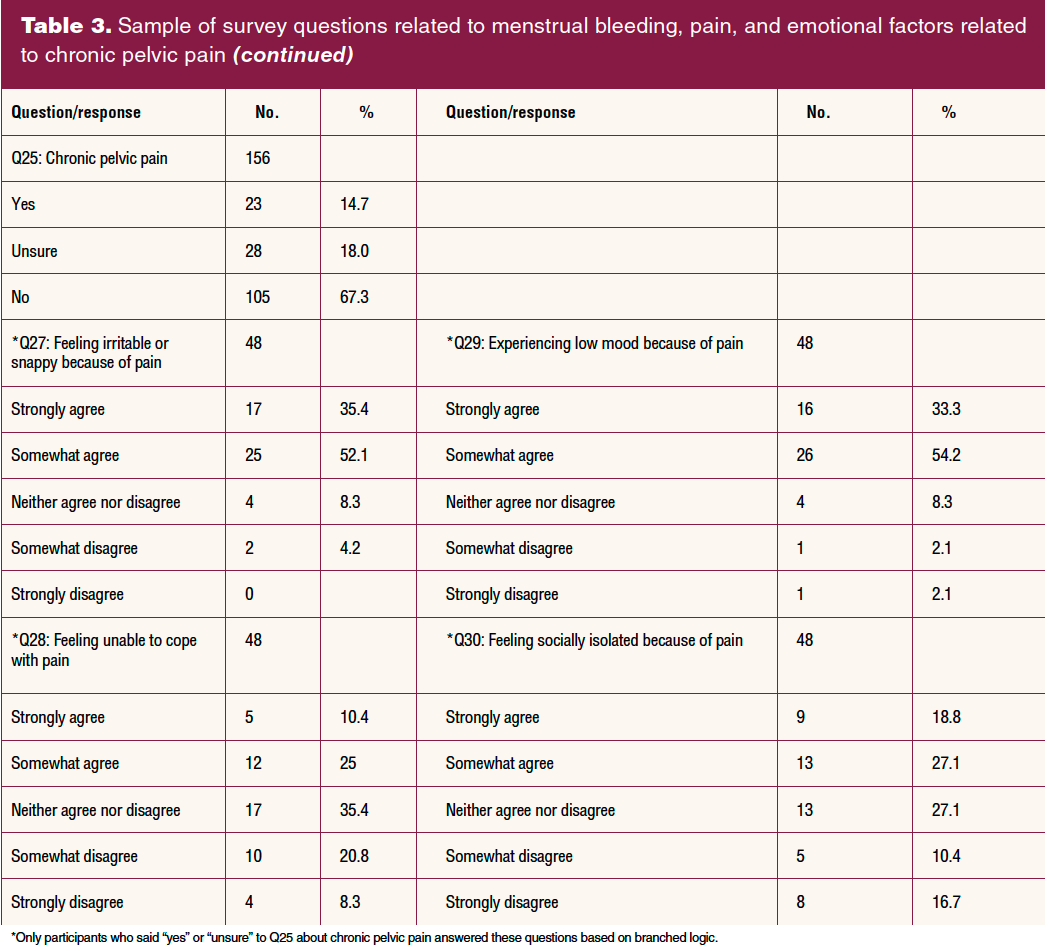
Survey questions related to menstrual pain, chronic pelvic pain (CPP), bleeding, and missed school and social activities are included in Table 3. A majority of participants described their periods as “moderate, heavy, or very heavy.” Most respondents answered in the middle range for pain, with a small percentage reporting no pain and a slightly higher percentage reporting severe pain. Approximately 18% reported having missed 1 to 3 days of work or school due to bleeding in the past 3 months. The number of days of social activities missed was much higher, with 37% reporting missing 1 to 3; 14% missing 4 to 8, and less than 1% missing 9 to 12 days in the last 3 months due to menstrual symptoms. Chronic pelvic pain was described in the survey as pain below your belly button and between your hips that continues for at least 6 months or longer, but the pain can come and go during that time. Almost 15% of respondents reported “yes” and 18% reported “unsure” to whether or not they believed they had CPP. Table 3 shows a sample of branched logic questions for those who said yes or unsure to CPP.
Focus group participants were asked to describe their biggest concerns about menstrual symptoms; if/how the symptoms influence relationships, school, and/or work; and whether or not self-care behaviors and monitoring of symptoms using an app-based tool were helpful. Questions about app-based tools were included based on knowledge that these were being used more by individuals to both track periods and engage in healthy exercise and eating behaviors.
Regarding symptoms, participants discussed having severe pain, irregular periods, excessive bleeding, mood swings, and anemia:
- There is anxiety with the pain management. I find that if I’m trying to do school or in class trying to focus, I can find it a huge distraction. Throws off your whole routine of the day.
- It makes me not want to do anything. It affects school, relationships, hormones.
Participants expressed their concerns about healthcare providers not listening to them and having to advocate for themselves. Participants explained feeling dismissed when tests came back “normal.” They expressed not being able to find time to see a healthcare provider. Stigma around family dynamics and how menstrual cycles and treatments are not talked about were mentioned:
- Last month, I needed to renew my birth control and I don’t really have a break for school that matched up with my doctor. They called me and said you need to come in for your yearly physical so we can renew your birth control. Birth control has worked phenomenally for me to work with menstrual symptoms and keeping them regular. When they are difficult about renewing it when you can’t get in, that is a big barrier.
- One barrier that arose for me when I was dealing with cycle issues is that I am from a small community and we didn’t have a specialist who could deal with my issues. I ended up needing to travel over 2 hours to see someone who could help and get me on the correct medication and management system to help with my cycle.
- For me, as a barrier in the Hispanic community, you are not supposed to talk to someone who is not your mom or another female figure in your household. If I had cramps, I wouldn’t tell my dad or uncle, just say I have a stomach ache. Growing up was very hard, especially when I was in middle school when I needed someone to pick me up from school. I couldn’t tell them what was really wrong.
Respondents reported how menstrual symptoms negatively shaped their health, happiness, and enjoyment, which are integral parts of their quality of life. This included always thinking about their menstrual cycle even when they are not experiencing symptoms. Concerns with mood swings and disruption of relationships were discussed:
- I would like to think that my symptoms do not impact my quality of life, but when I do have heavy periods, I get more anxious and think I might bleed through a tampon. Am I going to be on vacation when I get my period? Am I going to have pelvic pain when I’m out to dinner with friends? I get anxious.
- I think it impacts my quality of life since I’m always thinking about it. When is it going to pop up, am I going to miss something important?
The most common menstrual symptom relievers reported were over-the-counter pain medications, natural teas, hot packs, eating healthy, and exercise. Some stated that they do not use anything and just suffer through the pain. Many participants reported use of app-based tools to track timeliness and symptoms of their menstrual cycle. Some reported their choice was influenced by their culture:
- I’ve never had the same day, the same week, the same length of time. Trying to predict with other stressors. I have tried to record if it was a stressful time or if I’m eating things that I know irritate me. Dairy is one I avoid that does help with fewer cramps. I haven’t been able to find any correlation between stress and having my period. I think it’s been sort of helpful to track it, to have evidence that I’m not crazy.
- I have done research on my own and experimented. For me, eliminating foods that cause inflammation like dairy and gluten. Managing stress has helped.
- Even though this is something that I desperately do not want to suffer through, I think finding solidarity in finding groups like this.
Limitations
Study limitations included the diversity and locality of the sample size. The demographics of this sample appeared to be representative of college-age students in this setting. The survey used inclusive language about gender in the hope this would include anyone who has menstrual cycles or has had them but may not identify as female, such as those who are nonbinary, transgender, and gender nonconforming. It is possible that there was bias in those who replied to the survey and participated in the focus group, as they may have been more likely to reply if they experienced negative menstrual symptoms.
Discussion and implications for practice
The National Association of Nurse Practitioners in Women’s Health published a position statement on menstrual equity in 2022 that includes the importance of healthcare access for menstrual health, including associated physical, mental, and social well-being.15
The role of NPs is to create a safe environment for culturally congruent care. This includes a supportive space for individuals who are nonbinary or transgender and may be less comfortable discussing menstruation with friends and family. Having providers ask about these symptoms and provide resources could improve quality of life. Multiple participants mentioned that having had the opportunity to talk with others about their menstrual experience was in itself beneficial and therefore support groups and conversations led by NPs may assist in individualized plans and therapy.
Results showed symptoms influenced relationships. Focus group participants discussed how rumination of their menstrual cycles can affect their ability to focus on their relationships including enjoyment in dating or sexual activity. Some respondents reported pain caused them to avoid intimate relationships altogether, similar to other research findings that pain and bleeding influenced students’ social relationships with friends and family and caused hardships in their activities of daily living.16
Our survey and others found young adults miss school and social activities due to dysmenorrhea.6,9 Symptoms also negatively influenced the mental health of our respondents, especially related to low mood. Participants reported feeling alone in their struggles and uncomfortable sharing them with others, suggesting they may have felt resigned to their negative menstrual experiences. Other research has shown that women do not reach out for help with their menstrual problems but would prefer proactive support from their provider.11,12,17 Such findings have great implications for NPs to become more actively engaged and provide proactive support in the management of these young adults’ menstrual symptoms.
Barriers to menstrual healthcare were described. Participants expressed poor or nonexistent communication with their healthcare provider, feelings of dismissal and not being listened to, lack of access to care, and menstruation being considered a taboo topic within their families and/or cultural groups or that it could only be discussed with other women. An increase in health literacy related to menstruation and normalization of period talk is needed. Research has found that some women do not seek care because they assume their symptoms are normal and believe that providers will not help, or feel embarrassed and/or afraid to seek care.11,12 Providers could include health education about what is normal about menstruation in their visits with young adults. Young adults can be encouraged to seek both pharmacologic (eg, nonsteroidal inflammatory drugs and oral contraceptive pills) and nonpharmacologic (eg, physical activity, yoga aromatherapy, dietary changes) therapy to help with symptom relief.6,7 Providers are well poised to include assessment regarding access to and use of menstrual hygiene products to help manage physical, mental, and social symptoms.15 Having a provider who is willing to communicate on these sometimes taboo concerns may make clients more likely to communicate about other healthcare concerns, increasing client and NP trust. Investigators have discussed four ways providers can reduce stigma about menstrual health: examining one’s social positionality and how it affects their approach to communication, reflecting on and acting against implicit bias, becoming an advocate, and engaging in community-based research initiatives.12 Nurse practitioners are well positioned to promote advocacy for menstrual equity.
Conclusion
This study set out to explore quality of life of young adults in relation to their menstrual symptoms, and results showed negative impacts. The findings in this study provide insight into how young adults in one college setting experience menstruation and associated negative symptoms. Additional research that includes a more diverse representation of young adults who menstruate in both college settings and other environments is important. Transgender males and nonbinary people who menstruate should be included in this research as they face unique challenges in accessing nonjudgmental and nonstigmatizing menstrual healthcare. Quality improvement initiatives in clinical settings can focus on ensuring menstrual health is a topic that is consistently included in healthcare provider and client conversations. Nurse practitioners and other advanced practice registered nurses who provide women’s and gender-related healthcare can lead or partner with colleagues in these research and quality improvement endeavors, as well as provide a safe space for young adults to discuss their menstrual concerns
Catherine U. Graeve is a program director in the School of Nursing at St. Catherine University in St. Paul, Minnesota. Grace Gao is a RWJF Future of Nursing Scholar Alumni 2015–2018 and Associate Professor in the School of Nursing at St. Catherine University. Vera I. Stephenson is Assistant Professor in the School of Nursing at St. Catherine University. Rachel Helland was a research assistant and Master’s candidate at the time of this study, graduating from the Master of Public Health in Global Health program in the Henrietta Schmoll School of Health at St. Catherine University. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(4):34-41. doi: 10.51256/WHC082334
References
1 Davies J, Kadir RA. Heavy menstrual bleeding: an update on management. Thromb Res. 2017;151(suppl 1):S70-S77.
2 Allyn K, Evans S, Seidman LC, Payne LA. “Tomorrow, I’ll Be Fine”: impacts and coping mechanisms in adolescents and young adults with primary dysmenorrhoea. J Adv Nurs. 2020;76(10):2637-2647.
3 Rafique N, Al-Sheikh MH. Prevalence of menstrual problems and their association with psychological stress in young female students studying health sciences. Saudi Med J. 2018;39(1):67-73.
4 Sveinsdóttir H. Menstruation, objectification and health-related quality of life: a questionnaire study. J Clin Nurs. 2018;27(3-4):e503-e513.
5 Laksham KB, Selvaraj R, Kar SS. Menstrual disorders and quality of life of women in an urban area of Puducherry: a community-based cross-sectional study. J Family Med Prim Care. 2019;8(1):137-140.
6 Rajput V. An overview on dysmenorrhea. Int J Nurs Educ Res. 2021;9(3):381-384.
7 Tsonis O, Gkrozou F, Barmpalia Z, et al. Integrating lifestyle focused approaches into the management of primary dysmenorrhea: impact on quality of life. Int J Womens Health. 2021;13:327-336.
8 Armour M, Parry K, Al-Dabbas MA, et al. Self-care strategies and sources of knowledge on menstruation in 12,526 young women with dysmenorrhea: a systematic review and meta-analysis. PLoS One. 2019;14(7):e0220103.
9 Munro AK, Hunter EC, Hossain SZ, Keep M. A systematic review of the menstrual experiences of university students and the impacts on their education: a global perspective. PLoS One. 2021;16(9):e0257333.
10 Yonglitthipagon P, Muansiangsai S, Wongkhumngern W, et al. Effect of yoga on the menstrual pain, physical fitness, and quality of life of young women with primary dysmenorrhea. J Bodyw Mov Ther. 2017;21(4):840-846.
11 Chen CX, Shieh C, Draucker CB, Carpenter JS. Reasons women do not seek health care for dysmenorrhea. J Clin Nurs. 2018;27(1-2):e301-e308.
12 Casola AR, Kunes B, Jefferson K, Riley AH. Menstrual health stigma in the United States: communication complexities and implications for theory and practice. J Midwifery Womens Health. 2021;66(6):725-728.13-1.
13 The World Health Organization Quality of Life assessment (WHOQOL): development and general psychometric properties. Soc Sci Med. 1998;46(12):1569-1585.
14 Al-Abbadey M, Liossi C, Graham CA. The Impact of Female Chronic Pelvic Pain Questionnaire (IF-CPPQ): a validation study. Clin J Pain. 2019;35(7):602-610.
15 National Association of Nurse Practitioners in Women’s Health. Position Statement. Menstrual Equity. Womens Healthcare. 2021;9(6):18-22.
16 Hailemeskel S, Demissie A, Assefa N. Primary dysmenorrhea magnitude, associated risk factors, and its effect on academic performance: evidence from female university students in Ethiopia. Int J Womens Health. 2016;8:489-496.
17 Eising HP, Sanders YV, de Meris J, et al. Women prefer proactive support from providers for treatment of heavy menstrual bleeding: a qualitative study in adult women with moderate or severe Von Willebrand disease. Haemophilia. 2018;24(6):950-956.
KEY WORDS: menorrhagia, menstruation, dysmenorrhea, young adult, quality of life, psychological adaptation