
The average woman has a 12.3% lifetime risk of being diagnosed with breast cancer.1 The number of breast cancer survivors continues to increase because of advancements in early detection and successful treatment of the disease.1 This rise in survival rate is generating greater attention on post-treatment effects and the importance of evaluating quality of life (QOL) for these patients. Many women treated for cancer experience problems related to sexual health and intimacy in particular.2 High levels of evidence support screening breast cancer survivors for sexual dysfunction, which can improve patient satisfaction and QOL.3,4
Purpose
Sexual dysfunction is recognized as a major problem following cancer treatment, which leads to increased distress and decreased QOL.2,4 The primary goal of this scholarly project was to implement the Female Sexual Function Index adaptation for breast cancer patients (FSFI-BC), an evidence-based, validated tool to screen for sexual dysfunction among breast cancer survivors.3 The FSFI-BC is a 33-item screening tool that uses Likert-scale questions to assess aspects of sexual functioning such as changes after cancer, desire, lubrication, orgasm, pain, reasons for sexual inactivity, and distress regarding sexual functioning. Use of this screening tool gives breast cancer survivors the opportunity to identify a sexual problem they may be having, discuss it with their healthcare provider (HCP), and begin treatment for it if indicated.
Method
The institutional review board approved this quality improvement project. Patients meeting inclusion criteria received an information letter discussing the screening tool and project purpose at their clinic visit check-in. Inclusion criteria included female gender; English speaker; age, 18-80 years; reader on at least a fifth-grade level; and a personal history of breast cancer diagnosed at least 1 year previously. Participants could be of any race, ethnic group, marital status, or socioeconomic status. Consenting participants completed the screening tool and demographic information sheet (de-identified to maintain confidentiality) prior to seeing the HCP. The project leader scored the data based on clinical interpretation guidelines3 and shared results with participants during their visit. Participants who screened positive for sexual dysfunction were given the opportunity to discuss treatment options and referral to appropriate specialists.
Outcomes
During a 3-week data collection period, 49 of 66 patients who met inclusion criteria participated in the project. Among the 49 participants, 4 (8.2%) were excluded because of missing data and 5 (10.2%) had sexual functioning that was equal or superior to that prior to their diagnosis. The remaining 40 participants (81.6%) met criteria for further evaluation based on FSFI-BC scores. Among these 40 participants, 22 (55%) were not distressed about their sexual functioning, 12 (30%) were distressed about their sexual functioning at least half the time, and 6 (15%) were excluded for missing data regarding distress (Figure).
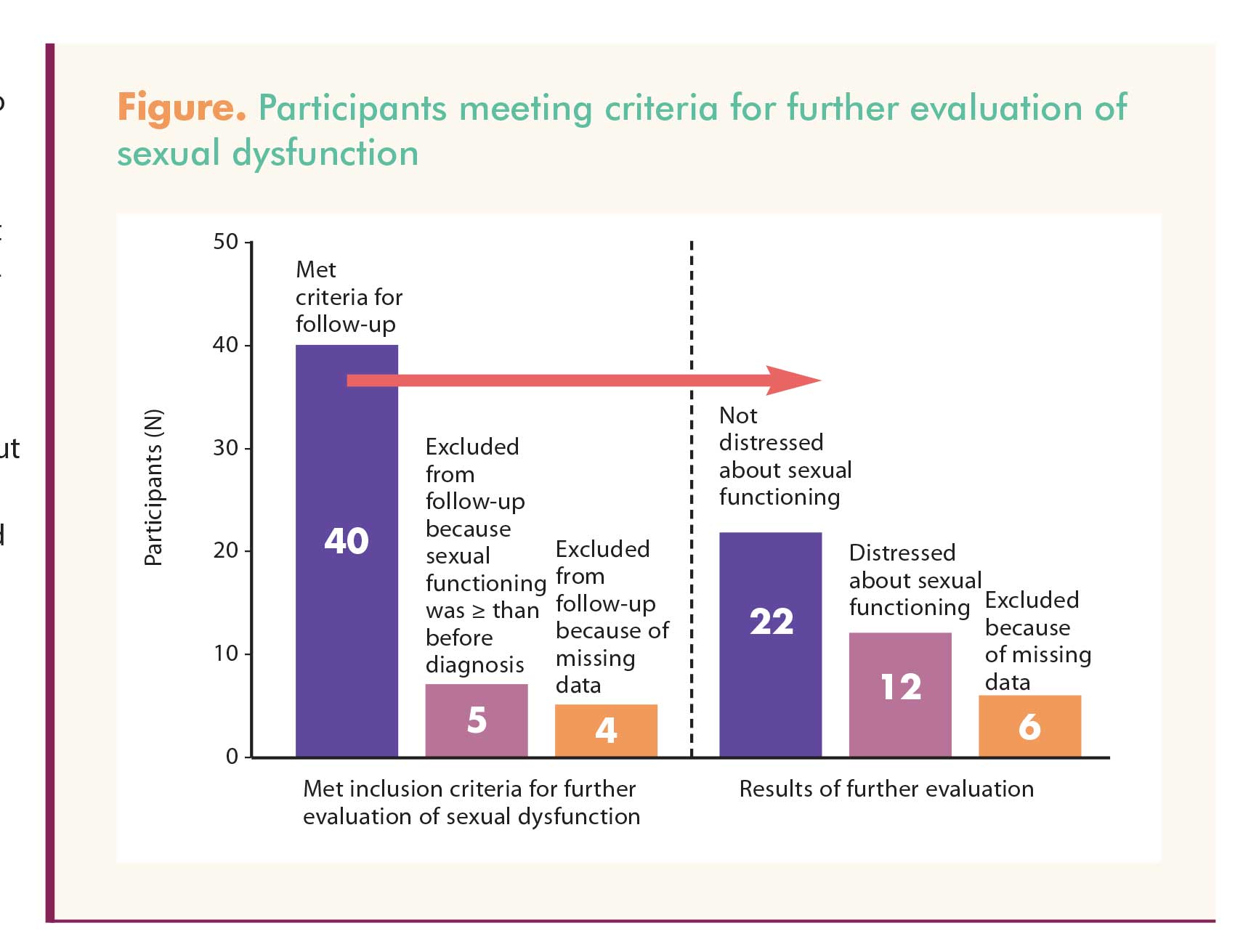{kind=link}
Limitations
The project was limited by the short interval for implementation and by incomplete surveys, which limited comparison of different facets of sexual dysfunction. In addition, the limited time frame for implementation did not allow for follow-up evaluation of outcomes for treatment recommendations or referrals made.
Implications for women’s health
Advanced practice nurses (APNs) serve a critical role in the comprehensive care and support of breast cancer survivors. Identification of sexual dysfunction is key to the evaluation and management necessary for survivors’ improved health outcomes. This project supports use of the FSFI-BC by APNs in identifying survivors with sexual dysfunction. In addition, APNs who perform this screening should have the knowledge and skills to address sexual function concerns and/or make appropriate referrals.
Stefani E. Davis is an advanced practice provider at OhioHealth Breast & Cancer Surgeons in Columbus, Ohio. Karen A. Hande is Assistant Professor and Ginny Moore is Assistant Professor and Director for the Women’s Health Nurse Practitioner Specialty, both at Vanderbilt University School of Nursing in Nashville, Tennessee. The authors state that they do not have a financial interest in or other relationship with any commercial product named in this article.
References
1. Desantis C, Ma J, Bryan L, Jemal A. Breast cancer statistics, 2013. CA Cancer J Clin. 2013;64(1):52-62.
2. Dizon DS, Suzin D, McIlvenne S. Sexual health as a survivorship issue for female cancer survivors. Oncologist. 2014;19(2):202-210.
3. Bartula I. Sherman KA. Development and validation of the female sexual function index adaptation for breast cancer patients (FSFI-BC). Breast Cancer Res Treat. 2015; 152(3):477-488.
4. Jeffery DD, Barbera L, Andersen BL, et al. Self-reported sexual function measures administered to female cancer patients: a systematic review, 2008-2014. J Psychosoc Oncol. 2015;33(4):433-466.
5. Cole CF. Breast cancer survivor satisfaction with NP-delivered follow-up care. Womens Healthcare. 2013; 1(1):16-21.