
Sexual violence is a public health issue defined by the Centers for Disease Control and Prevention as “sexual activity when consent is not obtained or freely given” and can affect people of all genders, races, and ages.1 Patients seeking healthcare after sexual violence often experience complex emotional reactions and heightened vulnerability, and their healthcare provider may be among the first to whom they disclose the event.2 Positive experiences with external support systems may help to facilitate recovery, whereas negative experiences with these systems can further the detrimental effects on a patient’s wellbeing.3 Competent healthcare providers for this population must incorporate trauma-informed care (TIC), including assessment and treatment options, reporting and legal advocacy options, and community resources available to the patient.
Project purpose
The purpose of this program development and implementation project was to improve clinician workflow at Planned Parenthood of the Pacific Southwest (PPPSW) to better care for and meet the needs of patients who present for care and counseling regarding legal and advocacy options following an event of sexual violence. A preliminary needs assessment indicated that providers often felt inadequately prepared to care for these patients. This project explored the clinician experience with sexual assault care before and after implementation of a workflow checklist and resource guide.
Description of setting/population
Project participants were recruited via email communication and follow-up word-of-mouth encouragement. Eligible clinicians from the 11 PPPSW family planning clinics in San Diego County were emailed about participating in the study, with 32 clinicians from 10 clinics opting in. Of participating clinicians, 23 were nurse practitioners and nine were physician assistants. One participant identified as male, and the other 31 participants identified as female. Four clinicians reported that they had previously worked in a setting where they regularly saw patients for sexual assault care. The range of experience in self-reported years working at PPPSW was 6 months to 23 years, with the average experience being 4.8 years at PPPSW.
Description of intervention
The resource guide was created with input from PPPSW’s Care Coordination Program Manager and community stakeholder organizations for sexual assault survivor advocacy. It also included aggregated information available online regarding local sexual assault examination sites and law enforcement information such as mandatory reporting requirements and child abuse reporting resources. The clinician workflow checklist was based on PPPSW clinical protocol and is included in the Figure.
Figure. Clinician workflow checklist
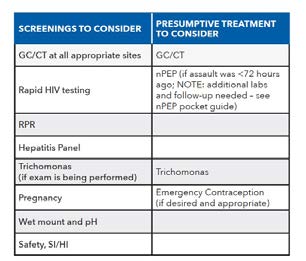
Discuss incubation period; advise patient to return to clinic in 4-6 weeks for
re-testing
CT, chlamydia; GC, gonorrhea; HIV, human immunodeficiency virus; nPEP,
nonoccupational HIV postexposure prophylaxis; pH, potential hydrogen; RPR,
rapid plasma reagin; SI/HI, suicidal ideation/homicidal ideation.
Methods to evaluate outcomes
This study was deemed “non-research” by the Vanderbilt Institutional Review Board and was approved by Planned Parenthood Federation of America. Participants took an anonymous pre-survey via Research Electronic Data Capture (RED-Cap) regarding their comfort with referrals of sexual assault patients and their current satisfaction with the workflow of sexual assault care visits. They were then given the workflow checklist and resource guide and asked to refer to it whenever they cared for a patient who presented for sexual assault care during the 6-week implementation period in the fall of 2019. Participating clinicians were asked to track how many occasions during the study time period they saw a patient for sexual assault care and utilized the workflow checklist and resource guide. After the implementation period, participants took a post-survey. The post-survey included questions about the usefulness of the clinician tool in improving workflow and increasing clinician comfort with referral resources. A thorough review of the literature on provider satisfaction and TIC revealed no previously validated tools that assessed the concepts of this study in the setting of outpatient, nonforensic sexual assault care. The surveys included demographic questions and five-point Likert scale questions. One survey question was borrowed from a previously used tool in the literature.4 The rest of the survey questions were created based on areas of desired improvement identified by clinicians during an initial needs assessment in the planning phase of this study. The REDCap survey was designed such that pre- and post-survey data could be matched with the same clinician while still anonymizing responses. The non-demographic survey questions can be found in Table 1.
Table 1. Survey
- I feel comfortable providing trauma-informed care.
- I am confident in my ability to interact sensitively with a patient who has a history of traumatic events.
- I feel stressed when caring for patients who have been sexually assaulted.
- I am satisfied with my ability to care for patients who have been sexually assaulted.
- I often feel as though I forget or miss things when caring for a patient who has been sexually assaulted.
- I know what to tell a patient to expect if they choose to present for a Sexual Assault Response Team (SART) exam.
- I am familiar with California state laws regarding mandatory reporting.
- I know what to expect if law enforcement is called to the clinic to help my patient report a sexual assault.
- I would like more support regarding community resources for patients who have been sexually assaulted.
- I am satisfied with the workflow of visits for patients who have been sexually assaulted.
- I would like more training regarding trauma-informed care.
- I found that the clinical checklist improved my workflow when caring for patients who had been sexually assaulted. (post-survey only)
- I found the community resource guide increased my comfort with referral resources related to sexual assault. (post-survey only)
Outcomes
Participants were divided into two groups. Group 1 was comprised of clinicians who reported on the post-survey that they saw at least one patient for sexual assault care (n = 13), and Group 2 was clinicians who reported that they did not see any patients for sexual assault care (n = 19) during the implementation period.
Due to the limited scope of this project and its intent to show clinical practice improvement over formal statistical improvement, data analysis focused on descriptive statistics. Likert scale results were converted from “strongly disagree,” “disagree,” “neutral,” “agree,” and “strongly agree” to numeric values from 1 to 5, respectively. The mean scores and standard deviation for responses to each pre-implementation survey question for both groups are in Table 2, along with the mean change in each question in the post-implementation survey for group 1. A positive mean change indicates an increase in agreement over time from pre-implementation to post-implementation, whereas a negative mean change indicates a decrease in agreement over time.
Table 2. Mean scores, standard deviation, and mean change in agreement on pre- and post-implementation survey questions
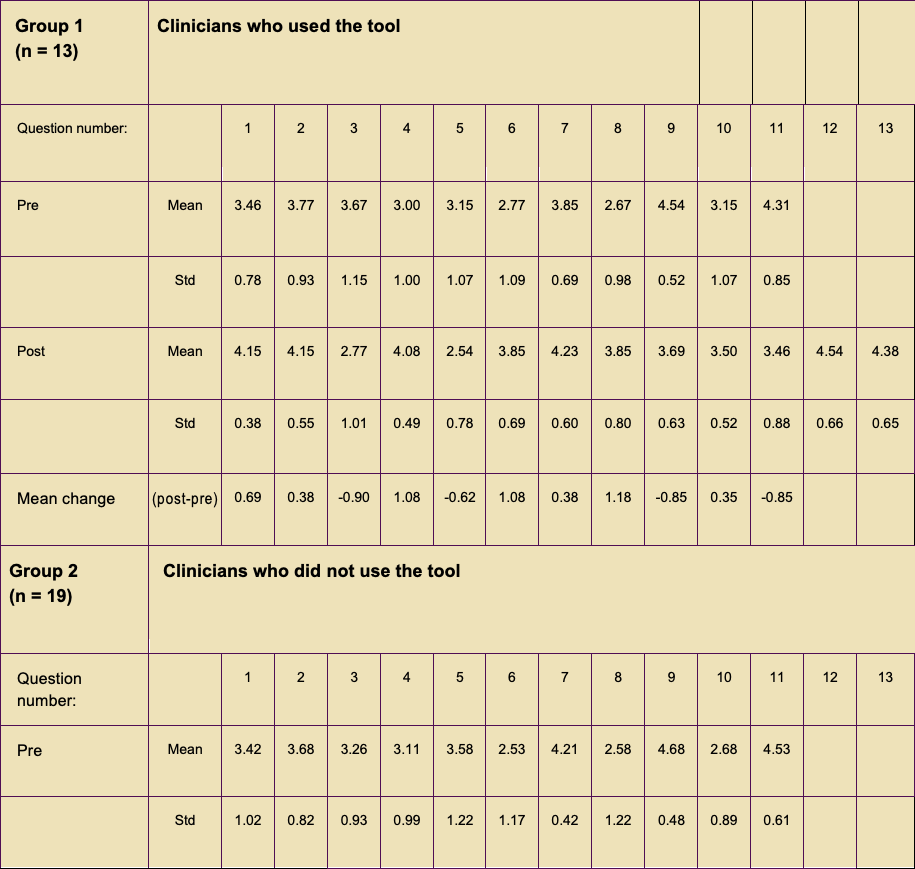
Std, standard deviation.
The changes observed are not statistically significant. However, clinically relevant change was observed. Of note, two questions that indicated meaningful change were Question 3, “I feel stressed when caring for patients who have been sexually assaulted,” with a -0.90 mean decrease in agreement, and Question 4, “I am satisfied with my ability to care for patients who have been sexually assaulted,” with a 1.08 mean increase. These changes demonstrate clinically relevant improvements in clinician comfort and satisfaction with sexual assault care after use of the clinician tool created for this project.
Table 3 shows a subgroup analysis of Group 1 that examined changes in mean scores among clinicians who had been at PPPSW for 3 years or less (“new clinicians,” n = 6) versus clinicians with more than 3 years of experience at PPPSW (“experienced clinicians,” n = 7).
Differences in mean changes when compared between subgroups of new versus experienced clinicians showed greater improvement reported among newer clinicians for nearly every question.
Table 3. Mean changes in survey agreement by question among clinician tool users (Group 1) based on years of experience at PPPSW
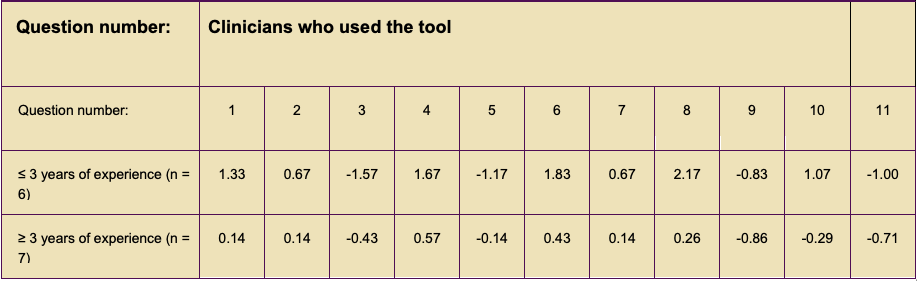
SPPPSW, Planned Parenthood of the Pacific Southwest.
Discussion
The results from this project show improvements in clinician satisfaction and comfort in the provision of sexual assault care as a result of the intervention and indicate that the project’s aims were met and improvement was made in clinician experience with sexual assault care at PPPSW. This is evidenced most strongly by the stark improvements in clinician report of decreased stress in responses to Question 3 and in increased satisfaction indicated by clinician responses to Question 4. This clinician tool has continued to be used at PPPSW and has become a part of onboarding materials for all new clinicians.
Conclusion
Limitations of this project include: small number of participants (N = 32) and short time scale (6-week implementation period). Additionally, there was no way to predict when a patient might present for the kind of sexual assault care that this project was designed to improve.
The clinician tool designed and used in this project is an example of a way in which a checklist and community resource guide can improve provider compliance with recommended care guidelines for sexual assault while also improving workflow and clinician experience. This has the further potential to provide patients with high-quality TIC experiences, which can positively impact their health outcomes and levels of empowerment as they navigate the healthcare system following an event of sexual assault. Finding the right fit for a clinician tool to improve sexual assault care in one’s community is an endeavor worth undertaking for its vast potential in improving the lives and health outcomes of these patients.
Elizabeth L. Howland is a nurse practitioner at Women & Infants Hospital of Rhode Island and a teaching associate at Warren Alpert Medical School of Brown University in Providence, Rhode Island. Carol C. Ziegler is Professor at Vanderbilt University School of Nursing, Vanderbilt Institute for Global Health, and co-founder of Climate, Health, and Energy Equity Lab at the W’Ondry, at Vanderbilt University in Nashville, Tennessee. Ginny Moore is Professor and Director of Women’s Health/Gender-Related NP Specialty at Vanderbilt University School of Nursing. The authors have no actual or potential conflicts of interest in relation to the contents of this article. The findings and conclusions in this article are those of the authors and do not necessarily reflect the views of Planned Parenthood Federation of America, Inc.
Funding information: The printing costs of the workflow checklist and resource guides produced and used for this project were generously included in the clinical services budget at Planned Parenthood of the Pacific Southwest.
Womens Healthcare. 2023;11(6):38-IBC. doi: 10.51256/ WHC122338
References
1 Centers for Disease Control and Prevention. Fast Facts: Preventing Sexual Violence. July 7, 2022. https://www.cdc.gov/violenceprevention/sexualviolence/fastfact.html.
2 Wadsworth P, Eve Krahe JA, Searing K. Health care seeking and engagement after sexual assault. J Nurse Practitioners. 2019;15(10):801-805.
3 Dworkin ER, Brill CD, Ullman SE. Social reactions to disclosure of interpersonal violence and psychopathology: a systematic review and meta-analysis. Clin Psychol Rev. 2019;72:101750.
4 Kis A. An Evaluation of Implementing Trauma-Informed Care Training in Healthcare Settings. University of Nebraska Medical Center, 2018.