
Women’s health behaviors during pregnancy may negatively or positively affect maternal and fetal/neonatal outcomes.1 Health behaviors during pregnancy that are likely to lead to positive outcomes—that is, health-promoting behaviors—include obtaining early prenatal care; acquiring pregnancy/childbirth education; adhering to nutritional and weight-gain guidelines; getting regular exercise and adequate sleep; avoiding use of tobacco, alcohol, illicit drugs, and certain over-the-counter drugs; avoiding engaging in risky sexual behaviors; reducing stress; and avoiding exposure to communicable infections.1,2 Might the type of prenatal care that a woman receives affect the likelihood that she will engage in health-promoting behaviors during pregnancy? And will these health-promoting behaviors then have a favorable impact on pregnancy outcomes?
Traditional prenatal care versus group prenatal care
Traditional prenatal care
Traditional prenatal care (TPC) occurs in a one-on-one setting between a patient and her healthcare provider (HCP). The emphasis is usually on early detection and intervention for health problems (e.g., hypertension, diabetes) that could adversely affect pregnancy outcomes.
Group prenatal care
Over the past two decades, group prenatal care (GPC) has emerged as an effective alternative to TPC.3 The CenteringPregnancy (CP) model, an evidence-based form of GPC, was developed by nurse midwife Sharon Rising in 1998.3,4 With CP, the emphasis is on education and peer support in addition to assessment.4,5 At each CP visit, 8-12 participants who are at similar points in their pregnancies check their own weight and blood pressure (BP), see an HCP on an individual basis for assessment of fetal heart tones and fundal heights, and then attend an educational group session that lasts about 90 minutes.
The group attends a total of 10 sessions together. Topics typically covered during these educational sessions include breastfeeding, common discomforts, comfort measures, family planning, mental health, personal goals, baby care and safety, intimate partner violence, and oral health.6
Literature review
A review of the literature gleaned from the CINAHL database showed that GPC, when compared with TPC, provided for greater patient–HCP contact and equal or superior pregnancy health-promoting behaviors and birth outcomes.5 GPC, versus TPC, fostered improved health behaviors such as taking prenatal vitamins, attending prenatal care visits,7 and breastfeeding one’s infant,5,8,9 and extended the interpregnancy interval by reducing the number of acts of unprotected sex.10
Birth weight and gestational age at delivery are important health indicators for newborns. When compared with TPC, GPC had a favorable impact on these birth outcomes. Group visits were associated with longer gestations11 and fewer preterm births.5,8 Ickovics et al5 reported preterm birth rates of 9.8% among GPC participants and 13.8% among TPC participants. Grady and Bloom8 reported 50% lower rates of preterm birth and low neonatal birth weight among adolescents receiving GPC versus TPC. One study showed that GPC participants, relative to TPC participants, were less likely to give birth to small-for-gestational-age infants, although the rate of preterm birth was not lower with group care.10 GPC was also associated with higher overall birth weights and lower odds of very low neonatal birth weight and fetal demise.11
Hale et al12 found that GPC, when compared with TPC, was associated with a higher participation rate in postpartum family planning services, although Shakespear et al13 found that CP participants engaged in fewer health-promoting behaviors than did their TPC counterparts. Overall, no difference was found between CP and TPC groups regarding the number of behaviors changed during pregnancy.12 Trudnak et al7 found that, when compared with TPC participants, CP participants were more likely to obtain adequate prenatal care; however, these women were more likely to formula-feed their babies. Although GPC shows promising birth outcome results, some studies found no diff erence in birth weight or gestational age at delivery between women receiving GPC versus TPC.7,14,15 Overall, the literature results have been mixed and studies have been limited by small sample sizes.
Blended prenatal care
Studies have documented several barriers to implementing the CP model or other types of GPC in an office setting designed for TPC. These barriers include initial costs, training of staff , absence of institutional space, lack of educational resources, scheduling issues, and recruitment and retention of patients. 16-18 Implementing a blended model of prenatal care is one way to overcome some of these barriers.
With blended prenatal care (BPC), group visits—typically 3 visits instead of 10—are integrated into the schedule of individual visits.19 Advantages of BPC are that facilitators can customize their own teaching topics to the group’s demographics, the clinic can implement GPC with fewer staff members and lower costs than the CP model, and the group can include high-risk pregnant women because individual care is still provided. In 2014, Lathrop and Pritham20 piloted a BPC model entitled Healthy Pregnancy, Healthy Childbirth, Healthy Parenting (HPCP). HPCP incorporates one 90-minute educational group visit in each trimester to advance maternal knowledge of self-care during pregnancy/childbirth and of infant care. Using a novel 8-item questionnaire, Lathrop and Pritham found that HPCP had a favorable impact on all outcome measures of maternal knowledge acquisition, self-efficacy, and satisfaction.
The study
A key measure of the efficacy of prenatal care and childbirth education is whether they have a favorable effect on patients’ health-promoting behaviors both during pregnancy and following childbirth. The purpose of this descriptive study, conducted from January 2017 to October 2017, was to ascertain how a BPC model compared with TPC in terms of the performance of health-promoting behaviors and in terms of pregnancy outcomes among women in a large multisite obstetrics practice. Approval for this study was obtained from the University of Alabama Institutional Review Board.
Patients were recruited and enrolled for the study by various office staff members, including medical assistants, receptionists, and the researcher. Flyers advertising the study were placed in the waiting room and throughout the clinic. Once women consented to participate, simple random sampling was done to assign them to the BPC group (n = 36) or the TPC group (n = 39). Any pregnant woman aged 18-44 years who received prenatal care at the multisite clinic was eligible to participate in the research study. Exclusion criteria included first-trimester spotting, miscarriage, twin pregnancy, and acquisition of late prenatal care (defined as >14 weeks’ gestation at the initial obstetric visit).
Data collected from participants included demographic information (e.g., age, race, marital status, highest educational level, gravida/parity status), maternal health behaviors during pregnancy, and gestational age and weight of the neonate at birth. Additional maternal outcome data obtained were weight gain during pregnancy, attendance at a postpartum visit, feeding method, and postpartum contraceptive use.
The BPC model used in this study was guided by Lathrop and Pritham’s pilot study.20 This model consisted of three group prenatal visits (one per trimester) that were integrated into the TPC schedule of individual visits. TPC consisted of about 14 prenatal visits. BPC participants completed the HPQ-II at the beginning of the first group meeting and at the end of the third group meeting. TPC participants completed this questionnaire at their scheduled prenatal visits at 10-14 weeks’ gestation and at 30-34 weeks’ gestation.
The BPC participants met once each trimester in the waiting room of the obstetrics practice. Because BPC participants could attend one of five different meetings during each trimester, the specific participants varied at each meeting. Group visits began with participants (typically, 5-8 per group) checking in at the front desk. The medical assistant obtained and recorded each woman’s BP, urinalysis results, and weight. Fetal heart tones and fundal heights were assessed, as needed, by the nurse practitioner at each of the group visits. Classroom time, led by the researcher, consisted of 60 minutes of instruction provided by a PowerPoint video, handouts, and a guest speaker. An additional half hour was available for questions and discussion.
Results
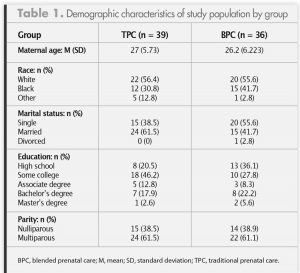
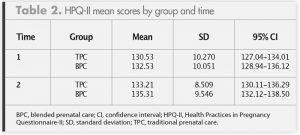
Table 1 provides demographic information about the two groups. Five women in the TPC group and four in the BPC group did not complete the third-trimester HPQ-II because of miscarriage, an out-of-state move, or a transfer of care. Therefore, a total of 66 women completed the first- and third-trimester HPQ-IIs. A mixed between-within ANOVA was performed to explore the effect of BPC on pregnancy health behaviors. Table 2 lists mean scores, standard deviations, and confidence intervals for the HPQ-IIs. Outcome variables were found to be normally distributed, and equal variances were assumed based on the results of Levene’s test F (1, 64) = 0.406 (P = .526) for time 1 score and F (1,64) = 0.223 (P = .631) for time 2 score. The interaction effect between performance of positive health behaviors and type of prenatal care was not significant, F (1, 1) = 1.038 (P = .312). There was a significant change in the performance of positive health behaviors over time for both groups based on Wilks’ Lambda = .93, F = (1) = 4.83 (P = .032), although the effect size was very small (multivariate partial η2 = .070).
 Maternal and birth outcome data are presented in Table 3. The groups did not differ significantly with respect to maternal weight gain, gestational age at delivery, or birth weight. Eight preterm births occurred in the TPC group and one
Maternal and birth outcome data are presented in Table 3. The groups did not differ significantly with respect to maternal weight gain, gestational age at delivery, or birth weight. Eight preterm births occurred in the TPC group and one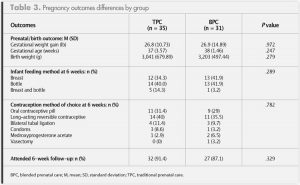 This study measured the performance of positive health behaviors prior to and following BPC versus TPC, and showed no significant difference between care models with respect to any health behavior scores. Both care models were found to be effective; significant and similar changes in health behavior scores occurred in both groups over time. From the first trimester to the third trimester, a nominal 3-point increase in mean score occurred in both groups. Although the two groups did not differ significantly in terms of gestational age or birth weight of their infants, the BPC group had only one preterm birth whereas the TPC group had eight such births.
This study measured the performance of positive health behaviors prior to and following BPC versus TPC, and showed no significant difference between care models with respect to any health behavior scores. Both care models were found to be effective; significant and similar changes in health behavior scores occurred in both groups over time. From the first trimester to the third trimester, a nominal 3-point increase in mean score occurred in both groups. Although the two groups did not differ significantly in terms of gestational age or birth weight of their infants, the BPC group had only one preterm birth whereas the TPC group had eight such births.Implications
- Lindgren K. Testing the Health Practices in Pregnancy Questionnaire-II. J Obstet Gynecol Neonat Nurs. 2005;34(4):465-472.
- March of Dimes website. Preterm Labor and Premature Birth: Are You at Risk? March 2018. marchofdimes.org/complications/preterm-labor-and-premature-birth-are-you-at-risk.aspx
- Bell KM. Centering Pregnancy: changing the system, empowering women and strengthening families. Int J Childbirth Educ. 2012;27(1):70-76.
-
Rising S. Centering pregnancy. An interdisciplinary model of empowerment. J Nurse Midwifery. 1998;43(1):46-54.
- Ickovics JR, Kershaw TS, Westdahl C, et al. Group prenatal care and perinatal outcomes: a randomized control trial. Obstet Gynecol. 2007;110(2 pt 1):330-339.
-
Centering Healthcare Institute website. Centering Pregnancy Overview. 2018. centeringhealthcare.org
- Trudnak TE, Arboleda E, Kirby RS, Perrin K. Outcomes of Latina women in CenteringPregnancy group prenatal care compared with traditional prenatal care. J Midwifery Womens Health. 2013;58(4):396-403.
-
Grady MA, Bloom KC. Pregnancy outcomes of adolescents enrolled in a CenteringPregnancy program. J Midwifery Womens Health. 2004;49(5):412-420.
- Brumley J, Cain MA, Stern M, Louis JM. Gestational weight gain and breastfeeding outcomes in group prenatal care. J Midwifery Womens Health. 2016;61(5):557-561.
-
Ickovics JR, Earnshaw V, Lewis JB, et al. Cluster randomized controlled trial of group prenatal care: perinatal outcomes among adolescents in New York City health centers. Am J Public Health. 2016;106(2):359-365.
- Tanner-Smith EE, Steinka-Fry KT, Lipsey MW. The effects of CenteringPregnancy group prenatal care on gestational age, birth weight, and fetal demise. Matern Child Health J. 2014;18(4):801-809.
-
Hale N, Picklesimer AH, Billings DL, Covington-Kolb S. The impact of Centering Pregnancy Group Prenatal Care on postpartum family planning. Am J Obstet Gynecol. 2014;210(1):50.e1-50.e7.
- Shakespear K, Waite PJ, Gast J. A comparison of health behaviors of women in centering pregnancy and traditional prenatal care. Matern Child Health J. 2010;14(2):202-208.
- Trudnak T. A comparison of Latina women in Centering Pregnancy and individual prenatal care. 2011. Doctoral dissertation, University of South Florida. scholarcommons.usf.edu.etd/3383
-
Kilma C, Norr K, Vonderheid S, Handler A. Introduction of CenteringPregnancy in a public health clinic. J Midwifery Womens Health. 2009;54(1):27-34.
- Novick G, Sadler LS, Knafl KA, et al. In a hard spot: providing group prenatal care in two urban clinics. Midwifery. 2013;29(6):690-697.
-
Novick G, Womack JA, Lewis J, et al. Perceptions of barriers and facilitators during implementation of a complex mode of group prenatal care in six urban sites. Res Nurs Health. 2015;38(6):462-474.
- Foster GA, Alviar A, Neumeier R, Wooten A. A tri-service perspective on the implementation of a centering pregnancy mode in the military. J Obstet Gynecol Neonatal Nurs. 2012;41(2):315-321.
-
Lathrop B. A systematic review comparing group prenatal care to traditional prenatal care. Nurs Womens Health. 2013;17(2):119-130.
- Lathrop B, Pritham UA. A pilot study of prenatal care visits: blended group and individual for women with low income. Nurs Womens Health. 2014;18(6):462-474.