
Lack of knowledge about human papilloma virus (HPV) has been cited as a barrier vaccination uptake. This study examines the effectiveness of two types of education on women’s intentions to become vaccinated against HPV.
The incidence of cervical cancer, a preventable disease, in the United States was 6.7 per 100,000 women in 2011, with a mortality rate of 2.3 per 100,000.1 Nearly all cervical cancers (99.7%) are caused by the human papillomavirus (HPV).2 Vaccination against HPV can prevent 90% of cervical cancers, but only 20% of U.S. women aged 19-26 years have received at least one dose of the vaccine.3 The author conducted a study to assess the usefulness of two educational interventions in increasing women’s knowledge about HPV and the Pap test, with the ultimate hope that this greater knowledge would translate into increased HPV vaccine uptake.
A systematic search of the health science databases Academic Search Premier, Women’s Health International, CINAHL, Medline, and PubMed was performed using the key words HPV, knowledge, beliefs, behaviors, education, prevention, and intervention to identify current research on educational intervention studies to promote HPV vaccination. Almost 5,000 articles were found. The search was then narrowed to English-language, scholarly, peer-reviewed studies with interventions aimed at females aged 13-64 years and published since 1999. After the limits were applied, 74 studies met inclusion criteria and were synthesized to draw conclusions about HPV knowledge and beliefs, women’s educational needs, and the types of educational interventions found effective at increasing HPV vaccine uptake among women.
A review of educational intervention studies suggested that lack of knowledge about HPV is a common barrier to HPV vaccine uptake.4-7 HPV knowledge tended to increase post-intervention. However, the studies all used only one educational approach to increase HPV knowledge. Most used written information alone; a few used oral presentations or videos. Some authors suggested that written material alone might not be as effective as verbal or video messages.8,9 To ascertain the usefulness of adding video messaging, the author compared the effectiveness of video plus written information with written information alone at increasing women’s HPV knowledge, Pap test knowledge, and vaccine intentions. Implications are drawn for future patient education strategies and healthcare provider (HCP) practice.
Method
Following acquisition of Internal Review Board approval, a quasi-experimental pre-test/post-test design was used. Participants were recruited from rural women’s healthcare clinics and via university email and Facebook. The prospective sample included 194 women aged 18-26 years who had not yet had the HPV vaccine. Women were excluded if they did not meet age criteria, were non-English speaking, were pregnant, or had received any HPV vaccinations. Participants were assigned to one of two educational interventions: (1) a written HPV factsheet created by the CDC (Group 1) or (2) a video containing HPV information and a cervical cancer survivor story plus the written HPV factsheet (Group 2).*
All participants gave written informed consent prior to completing the pre-test. Post-tests were administered 2 months after enrollment. A 2-month follow-up was chosen to allow time for participants to access the HPV vaccine series post-intervention, and to assess long-term HPV knowledge retention as a result of the educational intervention. Vaccine status was verified for all but 12 participants (6%) using a 3-step approach: chart audit, 42%; state immunization database, 39%; and self-report, 13%. Four participants in Group 1 and four in Group 2 received the HPV vaccine during the study period. Therefore, vaccine intention, rather than vaccine uptake, was evaluated as the study outcome variable. Intention to accept the HPV vaccine was determined based on a yes/no response to the question, “If cost were not an issue, would you accept the HPV vaccine for yourself?”
The instrument chosen for this study was used with permission from its designer, who confirmed its validity and reliability.10 The instrument is based on health belief model (HBM) constructs. Modifications of specific HBM constructs were made for this study; additional psychometrics are displayed in Table 1 and Table 2. Items assessing health beliefs were scored on a 4-point Likert scale, wherein 1 = strongly disagree and 4 = strongly agree. Other items on the instrument included history and demographic information to assess each participant’s sexual history, race, age, relationship status, and education level. In addition, 5 items assessed vaccine acceptability (e.g., Would you get a vaccine to prevent HPV infection?), 12 items assessed HPV knowledge, and 6 items assessed Pap test knowledge.
{kind=link}
{kind=link}
Results
Mean age of the 194 participants was 22 years. Most were white (n = 174); the remainder were black (n = 5), Hispanic/Latina (n = 4), Asian (n = 6), Native American (n = 1), or mixed (n = 4). Ninety-one participants were single, 84 were married and/or living with a partner, and 19 were in a relationship but not living with a partner. Ninety-one participants had attended some college, 45 had a high school diploma or GED, 36 had a bachelor’s degree, and 12 reported a graduate or professional degree.
Risk factors for HPV
Most participants had several risk factors for contracting HPV infection, including early age of sexual debut (mean age, 17 years), having >1 lifetime sexual partner (mean number of partners, 5), and not using condoms with their last act of sexual intercourse (proportion, 57%). In addition, 29 women older than 21 years reported never having had a Pap test. Among women who had undergone a Pap test, 38 had an abnormal result, with 19 knowing that the abnormality was a result of an HPV diagnosis, placing them at risk for developing cervical cancer.
HPV vaccine attitudes and perceived barriers
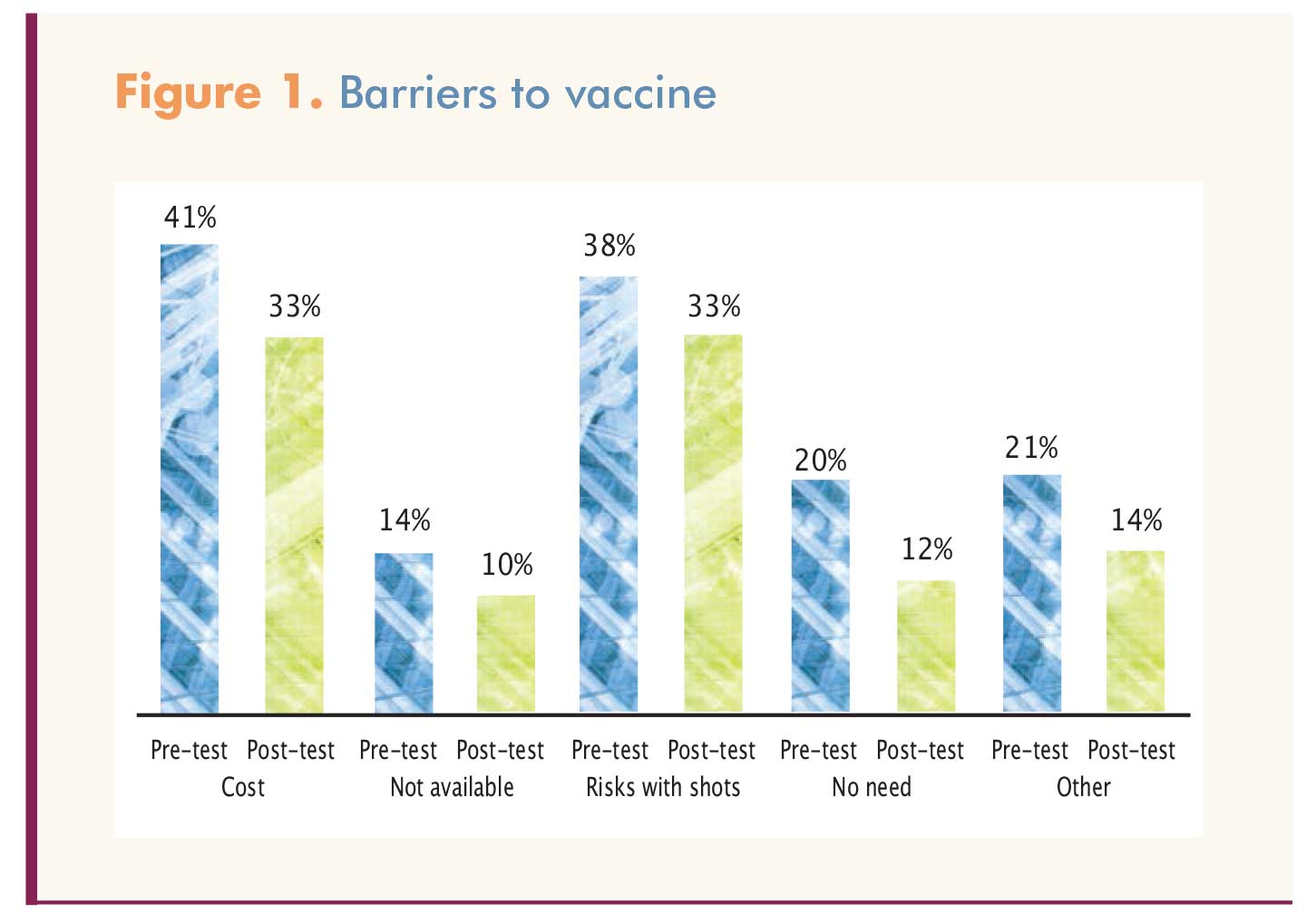
Reported barriers to getting the vaccine included cost, perceived risk, lack of availability, and lack of need for it. Figure 1 shows the percentage of participants who perceived these barriers before and after the educational intervention. The groups did not differ significantly in this regard, so the findings are reported as the total sample.
{kind=link}
HPV vaccine intentions
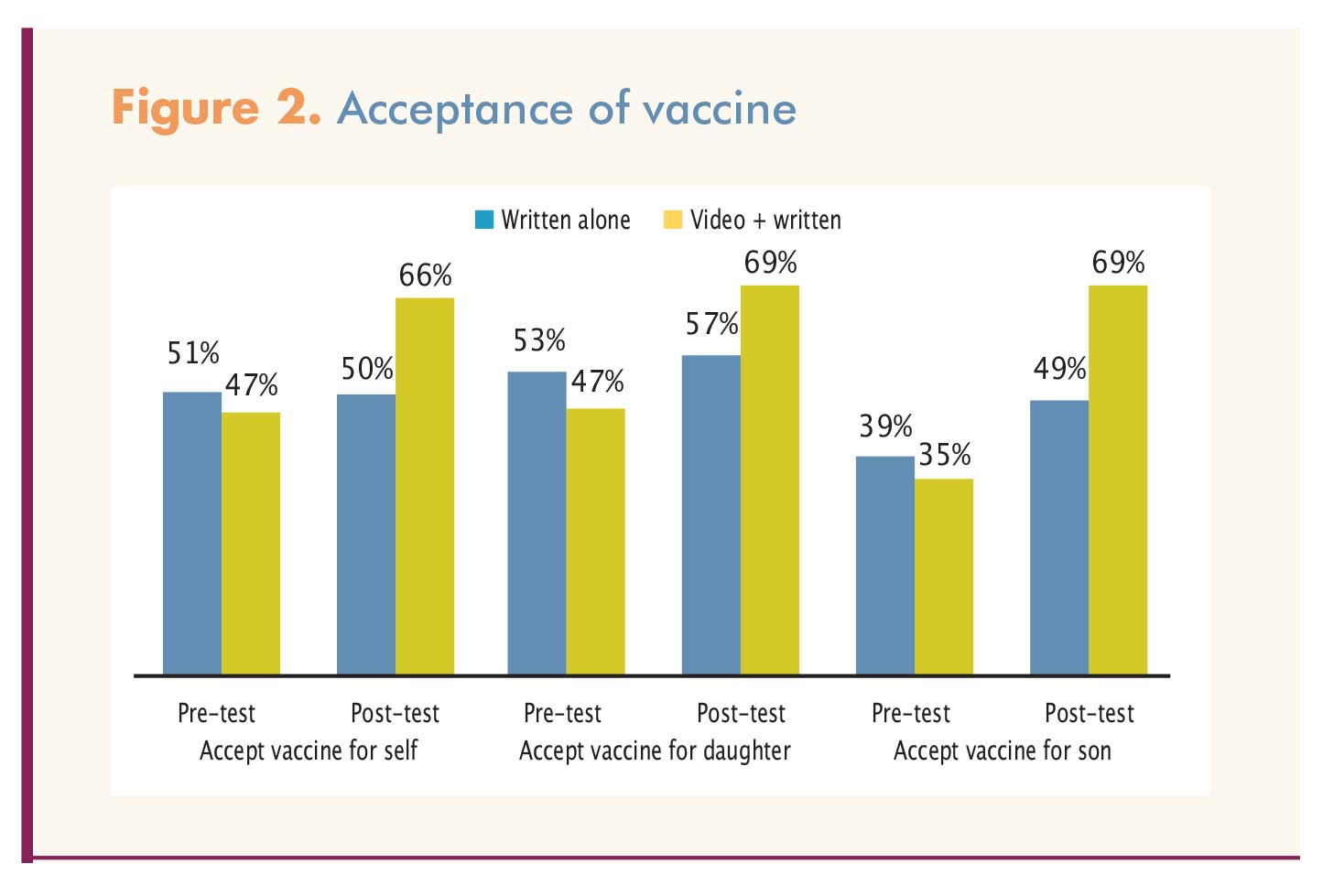
Before and after receiving the HPV educational intervention, participants were asked about their willingness to accept the HPV vaccine for themselves and, if they became parents, for their adolescent children. This willingness increased significantly in both Group 1 and Group 2, with no difference between groups in terms of their willingness to accept the vaccine for themselves or their adolescent daughters. However, after the educational intervention, participants in Group 2 were significantly more likely than those in Group 1 to say they would accept the vaccine for their adolescent sons (Figure 2).
{kind=link}
Knowledge scores
Participants were assessed on HPV and Pap test knowledge at baseline and at study completion. The groups did not differ on knowledge scores at pre-test or posttest, and both showed significant knowledge gains as a result of receiving education. This latter finding suggests that the two educational approaches (i.e., the factsheet alone vs. the video plus factsheet) did not differ in their effectiveness (Table 3 and Table 4).
{kind=link}
{kind=link}
Discussion
Impact on knowledge
The author hypothesized that the combination of a factsheet and a video-based first-person account story of a woman diagnosed with cervical cancer, with clear messages about prevention and treatment, would be a more powerful educational tool for increasing participants’ HPV and Pap test knowledge than a written factsheet alone. It turned out that knowledge increased significantly in both groups, and that the difference in knowledge gains between groups was not significant. This finding was similar to that of Krawczyk et al,11 who compared the efficacy of two HPV educational interventions, a pamphlet versus a video, in increasing HPV knowledge and vaccination intentions in college students. The investigators found that both educational interventions were similarly effective in this regard.11 The current study used a video that incorporated music, images, and cultural brokerage through a first-person account of a cervical cancer survivor. Although the difference between groups was not significant, Group 2 did have slightly higher knowledge scores than Group 1. It is unclear whether this slight edge was a result of the video messaging itself or the receipt of two educational strategies that reinforced each other.
At enrollment, participants’ HPV and Pap test knowledge levels were low, even among those who had regular contact with HCPs for Pap testing. This finding is consistent with the literature.12-16 Persistence of knowledge deficits despite increasing access to HCPs through the Affordable Care Act (ACA) speaks to unmet educational needs. Reasons for any woman’s knowledge deficits with regard to HPV and Pap testing, despite regular contact with an HCP, are unclear but may reflect a lack of time in the office for face-to-face education or an HCP’s lack of skill in imparting such information to a patient.17 In this study, 29 participants aged 21 or older reported never having had a Pap test. Lack of knowledge has been cited as a barrier to disease prevention-seeking behaviors such as getting a Pap test.18,19 Studies have shown that many women do not understand the purpose of a Pap test.20-22
Impact on HPV vaccination intentions
In this study, after the intervention, both groups were similarly and significantly more willing to accept the HPV vaccine for themselves and their adolescent children; Group 2 was significantly more willing than Group 1 to accept the vaccine for their adolescent sons. Evaluation of content in the two educational tools showed that the video may have been more gender neutral than the factsheet with regard to eligibility criteria for HPV vaccination. The video simply mentioned the ages for which the vaccine has FDA approval—“All males and females 9-26 years of age can receive the HPV vaccine”—whereas the factsheet was more specific about different age and risk groups who should be vaccinated.23
Although vaccination intentions increased, vaccine uptake during the study was not significantly affected; only 8 participants, 4 in each group, became vaccinated. Several barriers to vaccination might have influenced this finding. A major barrier was cost. Even though 84% of the participants reported having insurance coverage, nearly 41% of respondents on the pre-test and 34% of respondents on the post-test cited cost as a barrier to getting vaccinated. Although more young people are being insured through the ACA, there may be gaps in insurance coverage or lack of knowledge regarding vaccine coverage among the newly insured. Another barrier was access; many private HCP offices did not stock the vaccine. A third barrier may have been respondents’ lack of perceived need for the HPV vaccine. Some felt monogamy with a male partner or having a lesbian orientation eliminated the need. Others were at the end of the age bracket for HPV vaccination and did not seek to begin the vaccine series. A few reported prior diagnosis with HPV as a reason for not getting vaccinated. Finally, some participants had an inherent fear of all vaccines.
Limitations
Most study participants were white—the sample had little ethnic or racial diversity—and resided in rural Appalachia. Inferences about women from other ethnicities, races, or geographic locations cannot be made. Self-selection may indicate some bias by participants toward the topic, which would make their responses less representative of the population as a whole. Strict inclusion criteria for non-vaccinated participants prevented some age-eligible women from participating. Less stringent inclusion criteria might have provided interesting comparisons between vaccine-naïve and experienced participants. Finally, few participants became vaccinated during the study; therefore, conclusions can be drawn only regarding the impact HPV education had on intentions toward HPV vaccination.
Clinical implications
Nurse practitioners (NPs) are many patients’ first point of contact for healthcare information. NPs need to recognize that knowledge deficits regarding HPV and Pap testing exist, even among patients who visit regularly for Pap testing. NPs can aim to fill these gaps during every patient encounter. A simple factsheet can help fill the gap, but if NPs can provide educational videos to supplement the factsheet, patients may be even more motivated to get the HPV vaccine. NPs also need to remember that even if a given patient is older than 26, if she learns about the ability of the HPV vaccine to prevent cervical cancer, she will likely know that she should get her own children—including sons as well as daughters—vaccinated when they reach their preteen years. HPV vaccination is recommended by the American College of Obstetricians and Gynecologists, the American Academy of Family Physicians, the American Academy of Pediatrics, the CDC, and the Immunization Action Coalition.24 In addition to using educational tools to increase women’s knowledge about HPV and Pap testing, NPs can aim to overcome barriers to patients receiving the HPV vaccine by:
• helping insured patients understand that vaccines are covered by most insurance plans;
• helping uninsured patients by locating low- or no-cost vaccine options through state Vaccines for Children programs and pharmaceutical discount programs;
and
• dispelling fears and vaccine myths by distributing factsheets in their offices or clinics.
NPs can also try to disseminate information in places commonly viewed by the general public. This approach is important for women who do not undergo regular checkups. NPs need to try to reach these women where they live, work, shop, or travel to provide health information on the necessity of Pap testing and HPV vaccination.
More research on theoretically grounded educational interventions among differing populations at risk for HPV is needed. In particular, more research is needed to determine why women who have regular contact with HCPs lack knowledge about HPV and the HPV vaccine. In addition, more research is needed regarding gender bias in HPV vaccine recommendations. This study indicates a significant increase in women’s willingness to vaccinate adolescent sons following the video-based educational program. It is unclear whether the more gender-neutral video messaging was the cause of the discrepancy. Replication of this study among parents of adolescent children would help enhance NPs’ knowledge about adaptations that might be needed with regard to future HPV educational literature.
Crystal G. Sheaves is a Senior Lecturer at West Virginia University School of Nursing in Charleston. Financial support for this article was provided by West Virginia Immunization Network, a program of The Center for Rural Health Development, Inc.; and Sigma Theta Tau, Alpha Rho Chapter. The author states that she became a speaker for Merck & Co. after the study was conducted, and that Merck played no role in the funding of this study.
Acknowledgments
The author thanks Shalanda Bynum, PhD; Ilana Chertok, PhD; Stacey Culp, PhD; Marilyn Smith, PhD; Barbara Nunely, PhD; and Janie Leary, PhD, for their scientific guidance on the study.
References
1. Cervical Cancer Screening and Prevention. Practice Bulletin No. 157. Obstet Gynecol. 2016;127(1):e1-e20.
2. Ault KA. Epidemiology and natural history of human papillomavirus infections in the female genital tract. Infect Dis Obstet Gynecol. 2006;2006 suppl:40470.
3. CDC. Adult vaccination coverage – United States, 2010. MMWR Morbid Mortal Wkly Rep. 2012;61(4):66-72.
4. Mills LA, Vanderpool RC, Crosby RA. Sexually related behaviors as predictors of HPV vaccination among young rural women. J Womens Health (Larchmt). 2011;20(12):1909-1915.
5. Juraskova I, Bari RA, Obrien MT, McCaffery KJ. HPV vaccine promotion: does referring to both cervical cancer and genital warts affect intended and actual vaccination behavior? Womens Health Issues. 2011;21(1):71-79.
6. Mock J, McPhee SJ, Nguyen T, et al. Effective lay health worker outreach and media-based education for promoting cervical cancer screening among Vietnamese American women. Am J Public Health. 2007;97(9):1693-1700.
7. Patel DA, Zochowski M, Peterman S, et al. Human papillomavirus vaccine intent and uptake among female college students. J Am Coll Health. 2012;60(2):151-161.
8. Rosen NO, Knäuper B, Dio P, et al. The impact of intolerance of uncertainty on anxiety after receiving an informational intervention about HPV: a randomized controlled study. Psychol Health. 2010;25(6):651-668.
9. Waller J, Marlow LA, Wardle J. The association between knowledge of HPV and feelings of stigma, shame, and anxiety. Sex Transm Infect. 2007;83(2):155-159.
10. Bynum SA, Brandt HM, Friedman DB, et al. Knowledge, beliefs, and behaviors: examining human papilloma-virus-related gender differences among African American college students. J Am Coll Health. 2011;59(4):296-302.
11. Krawczyk A, Lau E, Perez S, et al. How to inform: comparing written and video education interventions to increase humanpapilloma virus knowledge and vaccination intentions in young adults. J Am Coll Health. 2012;60(4):316-322.
12. Cermak M, Cottrell R, Murnan J. Women’s knowledge of HPV and their perceptions of physician educational efforts regarding HPV and cervical cancer. J Community Health. 2010; 35(3):229-234.
13. Fry AM, Ferries-Rowe EA, Learman LA, Haas DM. Pap smear versus speculum examination: can we teach providers to educate patients? J Womens Health (Larchmt). 2010;19(9): 1715-1719.
14. Kahn JA, Slap GB, Bern stein DI, et al. Psychological, behavioral, and interpersonal impact of human papillomavirus and Pap test results. J Womens Health (Larchmt). 2005;14(7):650- 659.
15. Waller J, Marlow LA, Wardle J. Anticipated shame and worry following an abnormal Pap test result: the impact of information about HPV. Prev Med. 2009;43(5): 415-419.
16. Warren K. HPV knowledge among female college students and the short-term effectiveness of HPV education. Internet J Acad Phys Assist. 2010;7(2).
17. Bayer AM, Nussbaum L, Cabrera L, Paz-Soldan VA. Missed opportunities for health education on Pap smears in Peru. Health Educ Behav. 2011;38(2): 198-209.
18. Bynum S, Brandt HM, Friedman DB, et al. Knowledge, beliefs, and behaviors: Examining human papillomavirus-related gender differences among African American college students. J Am Coll Health. 2011; 59(4):296-302.
19. Juraskova I, O’brien M, Mullan B, et al. HPV vaccination and the effect of information framing on intentions and behavior: an application of the theory of planned behavior and moral norms. Int J Behav Med. 2012;19(4):518-525.
20. Hawkins NA, Cooper CP, Saraiya M, et al. Why the Pap test? Awareness and use of the Pap test among wom en in the United States. J Womens Health (Larchmt). 2011;20(4):511-515.
21. Panagopoulou E, Giata O, Montgomery A, et al. Human papillomavirus and cervical screening misconceptions undermine adherence. Am J Health Promot. 2011;26(1):6-9.
22. Vasconcelos CT, Pinheiro AK, Castelo AR, et al. Knowledge, attitudes, and practice related to the Pap smear test among users of a primary health unit. Rev Lat Am Enfermagem. 2011; 19(1):97-105.
23. CDC. Genital HPV Infection – Fact Sheet. Last updated May 19, 2016.
24. Give a strong recommendation for HPV vaccine to increase uptake!
*Note: This video was prepared, and the study was conducted, before the HPV 9-valent vaccine became available.