
Strategies to address weight loss and management are commonplace. Obesity rates continue to rise, particularly among women, and are associated with disease processes such as diabetes, cardiovascular disease, and gestational diabetes. Ketogenic nutrition therapy plans are becoming increasingly popular among patients and an area of opportunity for the women’s healthcare provider. Current data are limited on ketogenic nutrition in pregnancy, and it is therefore not recommended. It is important for clinicians to understand the basics of ketogenic nutrition plans and how their use can impact patient care outcomes beyond simple weight loss.
The reduced intake of carbohydrates as nutritional therapy in the clinical care approach has been used since the 1920s as therapy for epilepsy and later for diabetes before the discovery of insulin.1 Recently, there is evidence of ketogenic nutrition therapy resulting in diabetes diagnosis reversal, medication reduction, and insulin elimination over 2 years.2,3 A ketogenic nutrition plan involves daily intake of low amounts of carbohydrates. However, not all diets low in carbohydrates are ketogenic. The ketogenic nutrition plan is unique because it causes a metabolic shift of the body to use ketones (products of fatty acid metabolism) as a primary fuel source instead of glucose from carbohydrates. This natural physiologic state called nutritional ketosis or ketosis (blood ketone levels 0.5 mmol/L–6 mmol/L) can occur in the presence of very low carbohydrate intake.4
It is important for the women’s health clinician to be aware of different nutritional strategies being utilized by patients to manage health status and promote optimal health. Ketogenic nutrition therapy is becoming increasingly popular. Patients may present telling you that they are interested in or already on a ketogenic nutrition plan. This article describes the basics of ketogenic nutrition therapy, discusses current knowledge about its effectiveness in managing health conditions and special considerations during pregnancy, and provides insight into the incorporation of ketogenic nutrition therapy in practice.
Ketogenic nutrition therapy
A ketogenic nutrition plan has been defined as daily carbohydrate intake of 20 to 50 g/day or less than 10% of the 2,000 kilocalorie diet, irrespective of nutritional ketosis.5 Metabolic variability of individuals is unique. Therefore, the definition of nutritional ketosis is based on the carbohydrate levels required to shift most individuals into ketosis.5 Considering a ketogenic nutrition plan for patients requires a personalization of the level of dietary carbohydrate intake, as there is no “one size fits all” plan. Personalization should be holistic and include an understanding of factors such as chronic medical conditions, medications taken, lactation status, and activity level to allow for a unique recommendation for carbohydrate and adequate protein intake needed to achieve and maintain nutritional ketosis.4
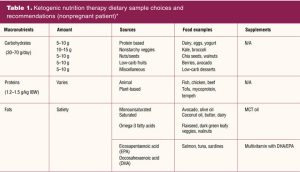
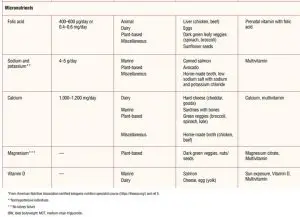
It is important to note that ketogenic nutrition therapy encourages a well-balanced, whole-foods eating approach contrary to “lazy keto,” which tends to include highly processed foods (ie, lunchmeats or fast food without bread). Ketogenic nutrition is not a diet, but a lifestyle change that incorporates the reduction of carbohydrates. A ketogenic nutrition plan should include low-carbohydrate foods, moderate protein, healthy fats, and balanced micronutrients.4 Table 1 provides a sample of healthy ketogenic food options. Paid resources from the American Nutrition Association ketogenic nutrition specialist course provide a summary of foods considered ketogenic friendly.4
The evidence for the therapeutic use of ketogenic nutrition plans in weight loss, improved cardiovascular risk factors, and reduction in type 2 diabetes is compelling. A recent systematic review and meta-analysis of low-carbohydrate diets including ketogenic nutrition plans showed that these improve metabolic and cardiovascular disease (CVD) risk factors in nonpregnant patients.6 Another recent systematic review showed that a ketogenic diet is effective in women to decrease weight and body mass index (BMI) and may be beneficial to reduce CVD risk factors.7 A 1-year nonrandomized controlled trial that included about 170 women diagnosed with type 2 diabetes showed a state of consistent nutritional ketosis as a result of a ketogenic nutrition plan improved glycemic control and biomarkers of CVD risk including weight, BMI, and blood pressure.2 Further, participants were able to reduce diabetes medications and insulin was reduced or eliminated in 94% of participants. A 12-month randomized parallel-group trial comparing a low-carbohydrate diet (< 40 g/day) to a low-fat diet in a diverse population of mostly Black persons (88% female; n = 66) showed a low-carbohydrate diet was more effective for reducing CVD risk factors and weight loss.8 The longest study examining consistent nutritional ketosis at 2 years noted beneficial effects on multiple clinical markers of diabetes (ie, fasting glucose or A1c) and cardiometabolic health (ie, decreased triglycerides and blood pressure), while utilizing less medications. The study also showed effectiveness in the resolution of diabetes and visceral diabetes with no adverse effects on bone health.3
Pregnancy considerations
A ketogenic nutrition plan is not recommended in pregnancy. However, there may be benefits to carbohydrate reduction in patients who are at risk for conditions such as gestational diabetes. High-quality research on outcomes in pregnant individuals who are on a ketogenic nutrition plan has been limited. Currently, there are only a few case studies published on ketogenic nutrition in pregnancy. More research and consensus are needed to determine how ketogenic diets during pregnancy affect human fetal brain development and other long-term healthcare outcomes.9 In studies with mice and other rodents with maternal ketogenic nutrition, their embryos grew quickly at first, then slowly resulted in smaller pups, decreased litter size, and retarded growth postnatally.9 Long-term effects of maternal ketogenic diets in humans are needed to further evaluate behavioral effects and cognitive or functional deficits that may occur later in fetal development.9
In pregnancy, macronutrient and micronutrient combinations are important to ensure the wellbeing of mother and fetus. The impact of adequate folic acid supplementation, for example, cannot be overemphasized. Adequate folic acid intake is associated with decreased neural tube defects (NTDs). Recent data from the Centers for Disease Control and Prevention reveal that 3,000 pregnancies per year are affected by NTDs in the United States, and worldwide more than 300,000 babies are born with an NTD.10 The current recommended intake for folic acid in women is 400 µg. For women with a history of neural tube disorders or a family history of NTDs, the recommended intake is 4 mg of folic acid starting at least 3 months prior to conception.11 Folic acid supplementation in women of childbearing years following a ketogenic plan is especially important because it has been noted that low carbohydrate diets, including ketogenic nutrition plans, may increase by up to 30% the risk for NTDs.12
For patients with or at risk for gestational diabetes mellitus (GDM), a reduction in carbohydrate intake is suggested. According to the 2022 American Diabetes Association (ADA) guidelines for management of diabetes in pregnancy, 175 g of carbohydrates are recommended, which is 35% of calories based on a 2,000 calorie diet.11 A systematic review of clinical practice guidelines for GDM noted the dietary recommendations varied and sometimes were contradictory. Most notably, specifics on dietary interventions, energy, and macronutrient intake were deficient.13 Whereas dietary interventions that reduce carbohydrate intake may be effective for treatment of GDM, data are not currently sufficient to advise ketogenic nutrition for this purpose during pregnancy. Pregnancy itself can cause an unintended state of ketosis for women due to physiologic changes and, in those with impaired insulin resistance, there is a risk for abnormally high levels of ketosis.14 Women’s health clinicians must be astute to the nutritional changes pregnant patients are making. Because ketogenic nutrition can be a lifestyle modification for some, patients may not mention this change to their provider. As part of the health history, clinicians should ask specifics about nutrition, calories consumed, and diet modifications made in order to ascertain these details. Nutrition conversation starters such as, “Tell me about the foods you usually eat?”, “Are there foods you tend to avoid?”, or “Do you think you eat a healthy diet? Why or why not?” can be used.15
Prepregnancy considerations–a scenario
Your 30-year-old patient presents for her annual exam. Her medical history is significant for gestational diabetes in her last pregnancy 2 years ago, which required diet changes only. You notice that the patient has had a 30-lb weight loss since her last office visit 12 months ago, at which time her BMI was greater than 30 (obese). She notes that she has been on a keto plan and loves the weight she has lost and how she now feels, noting increased energy, better moods, and improved sleep. She is currently taking a combination oral contraceptive pill. She takes no other medications and no vitamins or other supplements. Today, the patient’s BMI is 24 (normal).2 She tells you she is considering a pregnancy in the next few months and plans to discontinue her birth control pill next month. What prepregnancy assessment and counseling is important?
First, conduct a thorough assessment of the patient’s food intake and review weight gain goals during pregnancy, which is 25 to 35 lbs, based on her prepregnancy BMI. The patient should be advised to begin a prenatal vitamin with at least 400 µg of folic acid daily in the absence of any history of NTD. She can also be advised that foods such as green leafy vegetables, avocados, and brussel sprouts are high in folic acid and are acceptable choices on a ketogenic nutrition plan.4 Consider labs such a complete metabolic panel (CMP), thyroid-stimulating hormone (TSH) and HgbA1c to evaluate for nutritional deficiencies, thyroid disorders, and to screen for type 2 diabetes due to her history of GDM.
It is critical to discuss that data from current studies are insufficient to support the safety of a ketogenic nutrition plan during pregnancy. It is also important to maintain sensitivity for the patient’s wishes and utilize shared decision making throughout this process to develop a plan that incorporates the patient’s desires. If recommendations are made for alternative diet plans such as the Mediterranean or a vegetarian diet, it is important to consider a consultation with a dietician to ensure proper intake of adequate nutrients and/or need for supplementation of vitamins. If the patient expresses a desire to continue ketogenic nutrition during pregnancy, strongly consider consultation with a registered dietician (RD) or certified ketogenic nutrition specialist (CKNS) to discuss dietary strategies that may include a modified ketogenic nutrition plan. Developing an optimal nutrition plan for patients starts with an understanding of their baseline diet, what’s important to them, an assessment of psychological health (sleep habits, depression, anxiety, wellbeing), and addressing food security issues. Then we can recommend a customized plan, which may include referrals, that supports the patient’s desires and is one they can understand, follow, and maintain before, during, and after pregnancy.
Incorporating ketogenic nutrition therapy in practice
Healthcare clinicians can collaborate with an RD or CKNS to ensure optimal care for nonpregnant patients who may participate in a ketogenic nutrition plan. As BMI changes or blood pressure levels begin to normalize, it becomes necessary to evaluate current medications prescribed to ensure patients are not over treated and thus at risk for unintended adverse outcomes. Commercially available point-of-care capillary blood testing, urine dipstick, and breath test ketone meters can be used to monitor ketone levels to identify success with adherence and tolerance of a ketogenic diet. Beta hydroxybutyrate, a blood ketone, is considered a more accurate quantitative method of measuring nutritional ketosis.16 An individualized, patient-centered approach to care using shared decision making supports good clinical practice. Again, current data are insufficient to recommend ketogenic nutrition in pregnancy.
Many resources exist for clinicians interested in incorporating ketogenic nutrition therapy in practice. It is crucial to obtain formal training/continuing education around ketogenic nutrition science when looking to counsel or use a ketogenic diet as a means of nonpharmacologic therapy to improve diagnosed health conditions. It is important to understand the long-term impact of ketogenic nutrition on individual health outcomes. Clinicians must commit to a thorough understanding of physiologic changes and how they will impact medication management. Patient preferences, desires, and expectations are variable. There is no one-size-fits-all management plan.
The following can help provide guidance or additional education:
- Lowcarb.osu.edu: Ketogenic dietitian specialist service for personalized nutrition consultation
- Dietdoctor.com: Blog articles, videos, recipes, free limited edition, full access with subscription fee as a paid online resource
- VirtaHealth: Paid type 2 diabetes clinical management telemedicine service
- American Nutrition Association certified ketogenic nutrition specialist program: Renewable 5-year certification program offering two levels of training. Basic training for anyone and professional clinical application training for licensed clinicians
Life-long learning is needed to ensure knowledge on nutritional plans to provide the most comprehensive care to our patients before, during, and after pregnancy.
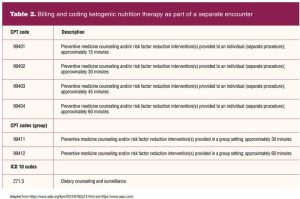
Reimbursement in practice for ketogenic or other nutrition management can be obtained through proper billing and coding (Table 2). This added skill enhances the scope of services the women’s health clinician can offer while generating additional revenue for a practice setting that bills a health insurance carrier. For settings caring for patients with inadequate or no medical insurance, a specialized program should be considered that is beneficial for the patient and practice setting.
Conclusion
As women’s health clinicians, we must be knowledgeable about lifestyle modifications that may impact a patient’s plan of care, including ketogenic nutrition plans. There is growing evidence to support the efficacy of ketogenic nutrition in some health conditions, but data are currently lacking to recommend this plan to pregnant and lactating women. It is important to recognize that there are specialty clinicians available to help with coordination of care in patients who choose ketogenic nutrition. Additional training is available for clinicians, such as nurse practitioners, who choose to increase their knowledge around ketogenic nutrition and become a direct provider for billable services that will generate additional patient revenue while meeting the unique needs of patients. Shared decision making helps maintain a therapeutic clinical relationship between provider and patient and should be utilized. Supporting health and wellness in patients is more than simply recommending exercise or calcium/vitamin D supplementation. A comprehensive and integrated approach to care is fundamental to the premise of WHNPs, and this methodology should motivate clinicians to continue with lifelong learning about new and evolving health practices.
Audra Hanners is Assistant Professor of Clinical Nursing and a certified ketogenic nutrition specialist at the Ohio State University College of Nursing in Columbus, Ohio. Angela D. Alston is Assistant Professor of Clinical Nursing, lead faculty-women’s health nurse practitioner specialty track, and Chief Diversity Officer at the Ohio State University College of Nursing. Dr. Hanners has grant funding from the Rita and Alex Hillman Foundation (GR118157) and Sigma Theta Tau International/American Nurses Credentialing Center (GR117688). The sponsors were not involved in the preparations, review, or approval of this manuscript. The project described was supported by a Path to K award from the Ohio State University Office of Health Sciences and the Center for Clinical & Translational Science. The content is solely the responsibility of the authors and does not necessarily represent the official views of the university or the Center for Clinical & Translational Science. Dr. Alston has no actual or potential conflicts of interest in relation to the contents of this article.
References
- Feinman RD, Volek JS. Carbohydrate restriction as the default treatment for type 2 diabetes and metabolic syndrome. Scand Cardiovasc J. 2008;42(4):256-63.
- Hallberg SJ, McKenzie AL, Williams PT, et al. Effectiveness and safety of a novel care model for the management of type 2 diabetes at 1 year: an open-label, non-randomized, controlled study. Diabetes Ther. 2018;9(2):583-612.
- Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-term effects of a novel continuous remote care intervention including nutritional ketosis for the management of type 2 diabetes: a 2-year non-randomized clinical trial. Front Endocrinol (Lausanne). 2019;10:348.
- Volek JS, Phinney SD, Krauss RM, et al. Alternative dietary patterns for Americans: low-carbohydrate diets. Nutrients. 2021;13(10):3299.
- Feinman RD, Pogozelski WK, Astrup A, et al. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition. 2015;31(1):1-13.
- Muscogiuri G, El Ghoch M, Colao A, et al. European guidelines for obesity management in adults with a very low-calorie ketogenic diet: a systematic review and meta-analysis. Obes Facts. 2021;14(2):222-245.
- Hanners A, Melnyk BM, Volek J, Kelley MM. Ketogenic diet, African American women, and cardiovascular health: a systematic review. Worldviews Evid Based Nurs. 2022;19(1):35-41.
- Bazzano LA, Hu T, Reynolds K, et al. Effects of low-carbohydrate and low-fat diets: a randomized trial. Ann Intern Med. 2014;161(5):309-318.
- Barry D, Ellul S, Watters L, et al. The ketogenic diet in disease and development. Int J Dev Neurosci. 2018;68:53-58.
- Centers for Disease Control and Prevention. Folic acid & neural tube defects: Data and statistics. 2021. Last reviewed: November 9, 2017.
- American College of Obstetricians and Gynecologists. FAQs. Nutrition during pregnancy. Updated March 2021.
- Desrosiers TA, Siega-Riz AM, Mosley BS, Meyer RE; National Birth Defects Prevention Study. Low carbohydrate diets may increase risk of neural tube defects. Birth Defects Res. 2018;110(11):901-909.
- Mustafa ST, Hofer OJ, Harding JE, et al. Dietary recommendations for women with gestational diabetes mellitus: a systematic review of clinical practice guidelines. Nutr Rev. 2021;79(9):988-1021.
- Qian M, Wu N, Li L, et al. Effect of elevated ketone body on maternal and infant outcome of pregnant women with abnormal glucose metabolism during pregnancy. Diabetes Metab Syndr Obes. 2020;13:4581-4588.
- Marshall NE, Abrams B, Barbour LA, et al. The importance of nutrition in pregnancy and lactation: lifelong consequences. Am J Obstet Gynecol. 2021;S0002-9378(21)02728-9.
- Lafountain RA, Miller VJ, Barnhart EC, et al. Extended ketogenic diet and physical training intervention in military personnel. Mil Med. 2019;184(9-10):e538-e547.
Key words: ketogenic nutrition therapy, ketogenic nutrition plans, neural tube defects, gestational diabetes mellitus
Womens Healthcare. 2022;10(4):29-37. doi:10.51256/WHC082229