
In the United States, female sterilization is relied on by 18.1% of women age 15 to 49.1 This prevalent method of permanent contraception is elected most frequently by women with lower incomes, those with public or no health insurance, women who are multiparous, those who are Black or Hispanic, and those with lower levels of education.2 The immediate postpartum period offers a safe time to proceed with permanent contraception with ease for clinical staff and convenience for the patient. Moreover, childbirth may be the only time some patients access care and premature resumption of sexual intercourse is common.2 Unfortunately, many women who desire postpartum sterilization do not obtain it. This article provides an overview of the Medicaid Requirements and Limits for Sterilization policy (42 Code of Federal Regulations, Part 441, Subpart F) with emphasis on the postpartum period, associated pros and cons, rulemaking recommendations, and implications for nurse practitioners (NPs).
Only 39% to 57% of those who request postpartum sterilization during prenatal care have the procedure.2 Contributing reasons include patient-related (ie, body mass index) and provider-related factors (ie, bias), scheduling/staff availability, receiving care at religiously affiliated hospitals, and bureaucratic regulations for consent and reimbursement by Medicaid.2 As such, approximately 50% to 60% of postpartum sterilizations requests go unfulfilled, often due to circumstances in which federal requirements have not been met.2–5 One study reported that more than two-thirds of unfulfilled requests were due to invalid Medicaid consents and that this group also had a low-likelihood of receiving interval sterilization.4 Those with high-risk pregnancies often request but do not receive the procedure.6 Women report feeling frustrated, angry, dissatisfied, and anxious about their inability to prevent repeat pregnancy.2
Historic and legal landscape of the policy
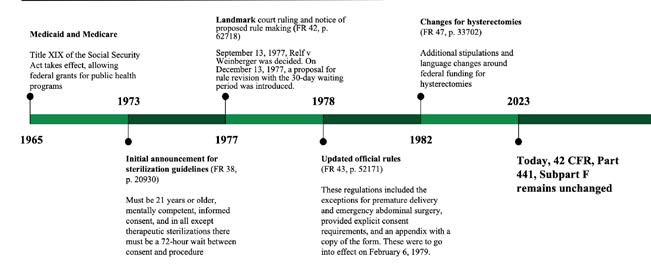
In the early 1900s, multiple states enacted eugenics laws that were upheld by the 1927 Supreme Court ruling in Buck v Bell.2,7 Involuntary sterilization was disproportionately inflicted on people of color, those with mental health conditions, those living in poverty, and those whose fertility was declared undesirable.2,7,8 This history of reproductive injustice continued in federally funded family planning programs in the 1960s and 1970s.2 In response to these wrongs, the Department of Health, Education, and Welfare began to regulate access to sterilization. In 1973, a 72-hour waiting period between consent and procedure was announced for all except “therapeutic” sterilizations.9 After the landmark case of Relf v Weinberger, a Notice of Proposed Rulemaking was published in the Federal Register in 1977 that extended this period to 30 days and it was acknowledged that the waiting period could create hardship.10 The historic timeline of the policy is further described in the Figure.
Figure. Historic highlights of Federal Regulation Title 42: Public Health, Subchapter C: MedicalAssistance Programs, Part 441: Services: Requirements and Limits Applicable to Specific Services,Subpart F: Sterilizations
Summary of the policy
Today the policy is under the control of the Department of Health and Human Services and applies to sterilizations and hysterectomies reimbursed by the Centers for Medicare and Medicaid. Federal financial participation is available for the sterilization of individuals only if they are at least age 21 years at the time of consent, they are deemed mentally competent, informed consent has been procured, and all criteria of the policy and state-level regulations have been met.11 People who are mentally incapacitated or institutionalized and those wanting hysterectomy with the lone purpose of sterilization are ineligible.11 Reimbursement is not available unless Medicaid has documentation proving all requirements are met.11 This includes the controversial mandated waiting period of 30 to 180 days to obtain the procedure after consent signature.11 The only exceptions to this waiting period are for preterm deliveries or emergency abdominal surgeries, which have a waiting period of 72 hours.11 The core tenets of this policy have remained unchanged since 1978.12
The policy has explicit components designed to safeguard informed consent and thwart coercion. Specific counseling topics include: the patient holds the right to withdraw consent at any time without loss of benefits, alternative contraceptives, guidance that sterilization is irreversible, applicability of the waiting periods, and explanation of the procedure and its associated risks and advantages.11 Translation and communication services should be provided, and a witness of the patient’s choice must be present.11 Informed consent is prohibited in times of physical or emotional distress, during labor/birth/abortion, or if the patient is under the influence of substances affecting their mental acuity or volition.11
The waiting periods
Critics of the policy argue that while initially benevolent, the waiting periods serve as a barrier to autonomously chosen care. Due to these time constraints, most individuals seeking sterilization would need to consent during a prenatal visit, which is not a universal experience as many face challenges accessing regular care.2,3,7 Although the 72-hour waiting period for preterm birth and emergency abdominal surgery is generous compared to 30 days, it still poses a barrier because these scenarios cannot be predicted. These patients may be offered an interval sterilization, but scheduling this outpatient procedure is problematic. If it has been longer than 180 days from consent signature, the patient will need to sign the consent again and the clock gets set for the 30 days once more. Still, in a total of 14 states where postpartum Medicaid coverage has not yet been extended to 12 months, the coverage period expires 60 days after birth and the family will be uninsured if they do not meet the state Medicaid eligibility levels.13
When announcing these rules, the agency admitted that “existing information does not permit precise predictions as to the effects of the proposed choices” and that while it was not believed that less than 30 days was inherently coercive, allowing additional time for patient reflection would offer risk mitigation.10 However, women who have undergone the procedure have been unable to cite any value of the rule, reporting that while it could be useful for other women’s decision making, it did not or would not affect their own choices.14 Regardless of insurance status, many women consider sterilization throughout their reproductive lives and are confident in this decision well before or shortly thereafter testing positive for their most recent pregnancy.14 Similarly, surveys of physicians who perform postpartum sterilization have mixed views on the power of the waiting period, with some considering it a discriminatory barrier, whereas others appreciate the historic origin and feel it protects autonomy.15
Public health and ethical impact
Unfulfilled sterilization requests contribute to unintended, short-interval, and high-risk pregnancies that are associated with adverse outcomes and morbidity and mortality.16–18 Almost half of women who do not obtain their postpartum sterilization may become pregnant within the next year.2,7,19 Those with public insurance are more likely than women with private insurance to have a short-interval pregnancy after an unfulfilled sterilization request.5,19 With the implementation of a revised Medicaid sterilization policy, it has been estimated that over 29,000 unintended pregnancies could be averted annually.7,20
Although states may adopt regulations for sterilizations, private insurance holders do not face the same barriers as the federally insured.2,7 Sterilization rates among Medicaid beneficiaries are low compared to those with private insurance, even after controlling for extraneous factors.21 When the sterilization interval was extended to 90 days’ postpartum, only 46% of Medicaid enrollees compared to 65% of privately insured women received sterilization.5 Most Medicaid subscribers identify as Black and Hispanic, and these women are more likely to be of fair or poor health, single mothers, of lower income, and not hold a high school diploma.22 Living in an area with increased neighborhood disadvantage is associated with worse fulfillment rates of desired postpartum sterilization for Medicaid beneficiaries compared to those with private insurance.23
Economic impact
Annual direct medical costs of unintended pregnancy in the United States were estimated to be at least $5.5 billion in 2018.24 A cost-effectiveness model demonstrated that when compared to the current policy, a revised version with reduced barriers to postpartum sterilization would increase fulfilled requests and save at least $215 million.20 Invalid Medicaid consent forms can lead to denied reimbursement for the costs of delivery and postpartum care, leaving the patient with a bill and/or driving up the hospital’s bad debt.2 Physicians fear ramifications and loss of funding if a postpartum sterilization is performed without valid Medicaid consent, yet few proceed due to a sense of ethical obligation.25
Rulemaking and solutions
Although the history of involuntary sterilization is critical to reflect on, it is imperative to consider changes to policies that, even when initially benevolent, currently obstruct patient sovereignty and advance inequity. An ideal policy should enhance sterilization fulfillment and respect women’s decision-making capacity while also ensuring informed consent. Policy recommendations include:
- Reduce the waiting periods by at least 50%: 14 days, with the exceptions of 24 hours for preterm births and a maximum of 6 hours for emergency abdominal surgery. Others recommend shortening the waiting period to 24 hours and extending the validity to 1 year.2
- Create a validated decision support tool.2
- Expedite surgery scheduling for interval sterilizations.2
- Expand Medicaid coverage to 12 months’ postpartum in states that have not yet done so.13
- Implement systems for tracking unfulfilled postpartum sterilizations at local, state, and federal levels.
- Implement hard-stop reminders via electronic medical record systems for counseling, consent signature, and procedure scheduling.
Implications for nurse practitioners
It is of utmost importance that NPs discuss postpartum contraception as early as the first trimester, especially if there is a threat of preterm birth, a cesarean delivery is anticipated, if the pregnancy is high risk, or if subsequent pregnancies pose extreme jeopardy. The patient may need to sign the consent form twice if completed early in pregnancy and 180 days are close to elapsing. For low-risk patients, NPs should consider performing counseling and signing the consent form at a standardized time during the pregnancy, such as between 24 and 28 weeks. NPs should stay vigilant for invitations for comment in the Federal Register or Unified Agenda, and advocate by writing petitions to the agency, submitting comments on Regulations.gov, requesting meetings with agency officials, and publishing op-eds in local media.26
Amanda Cassidy is a DNP graduate of Duke University School of Nursing in Durham, North Carolina, and a nurse practitioner at Columbia University Vagelos College of Physicians and Surgeons, Department of Obstetrics and Gynecology, Division of Maternal Fetal Medicine, in New York, New York.
Womens Healthcare. 2023;11(6):10-13. doi: 10.51256/ WHC122310
References
1 Daniels K, Abma JC. Current contraceptive status among women aged 15–49: United States, 2017–2019. NCHS Data Brief, no. 338. October 2020. https://www.cdc.gov/nchs/data/databriefs/db388-H.pdf.
2 American College of Obstetricians and Gynecologists. Access to postpartum sterilization. ACOG Committee Opinion no 827. Obstet Gynecol. 2021;137(6):e169-e176.
3 Wolfe KK, Wilson MD, Hou MY, Creinin MD. An updated assessment of postpartum sterilization fulfillment after vaginal delivery. Contraception. 2017;96(1):41-46.
4 Hahn TA, McKenzie F, Hoffman SM, et al. A prospective study on the effects of Medicaid regulation and other barriers to obtaining postpartum sterilization. J Midwifery Womens Health. 2019;64(2):186-193.
5 Arora KS, Wilkinson B, Verbus E, et al. Medicaid and fulfillment of desired postpartum sterilization. Contraception. 2018;97(6):559-564.
6 Albanese A, French M, Gossett DR. Request and fulfillment of postpartum tubal ligation in patients after high-risk pregnancy. Contraception. 2017;95(3):234-238.
7 Amalraj J, Arora KS. Ethics of a mandatory waiting period for female sterilization. Hastings Cent Rep. 2022;52(4):17-25.
8 Maykin MM, Pilliod RA, Werner EF. Discriminatory regulations on postpartum sterilization for Medicaid recipients propagate health inequities. Lancet Reg Health Am. 2021;6:100113.
9 Federal Register. 1973;38(149):20930-29031. https://www.govinfo.gov/content/pkg/FR-1973-08-03/pdf/FR-1973-08-03.pdf.
10 Federal Register. 1977;42(239): 62718-62732. https://archives.federalregister.gov/issue_slice/1977/12/13/62678-62855.pdf#page=35.
11 Code of Federal Regulations. Title 42 Part 441 Subpart F. Services: requirements and limits applicable to specific services. https://www.govinfo.gov/content/pkg/CFR-2021-title42-vol4/pdf/CFR-2021-title42-vol4-part441-subpartF.pdf.
12 Federal Register. 1978;43(217):52171-52173. https://www.govinfo.gov/content/pkg/FR-1978-11-08/pdf/FR-1978-11-08.pdf.
13 KFF. Medicaid postpartum coverage extension tracker. August 28, 2023. https://www.kff.org/medicaid/issue-brief/medicaid-postpartum-coverage-extension-tracker/.
14 Foley O, Janiak E, Dutton C. Women’s decision making for postpartum sterilization: does the Medicaid waiting period add value? Contraception. 2018;98(4):312-316.
15 Arora KS, Ponsaran R, Morello L, et al. Attitudes and beliefs of obstetricians-gynecologists regarding Medicaid postpartum sterilization – a qualitative study. Contraception. 2020;102(5):376-382.
16 Nelson HD, Darney BG, Ahrens K, et al. Associations of unintended pregnancy with maternal and infant health outcomes: a systematic review and meta-analysis. JAMA. 2022;328(17):1714-1729.
17 Hutcheon JA, Nelson HD, Stidd R, et al. Short interpregnancy intervals and adverse maternal outcomes in high-resource settings: an updated systematic review. Paediatr Perinat Epidemiol. 2019;33(1):O48-O59.
18 Centers for Disease Control and Prevention. Reproductive Health. Maternal Mortality. Pregnancy Mortality Surveillance System. Last reviewed March 23, 2023. https://www.cdc.gov/reproductivehealth/maternal-mortality/pregnancy-mortality-surveillance-system.htm.
19 Thurman AR, Janecek T. One-year follow-up of women with unfulfilled postpartum sterilization requests. Obstet Gynecol. 2010;116(5):1071-1077.
20 Borrero S, Zite N, Potter JE, et al. Potential unintended pregnancies averted and cost savings associated with a revised Medicaid sterilization policy. Contraception. 2013;88(6):691-696.
21 Morris J, Ascha M, Wilkinson B, et al. Desired sterilization procedure at the time of cesarean delivery according to insurance status. Obstet Gynecol. 2019;134(6):1171-1177.
22 Gomez I, Ranji U, Salganicoff A, Frederiksen B; KFF. Medicaid coverage for women. February 17, 2022. Women’s Health Policy. https://www.kff.org/womens-health-policy/issue-brief/medicaid-coverage-for-women/.
23 Arora KS, Ascha M, Wilkinson B, et al. Association between neighborhood disadvantage and fulfillment of desired postpartum sterilization. BMC Public Health. 2020;20(1):1440.
24 Filonenka A, Law A, Purser M, et al. Economic burden of unintended pregnancy in the United States. Poster presented at 2019 ISPOR 24th Annual International Meeting, New Orleans, LA; May 20, 2019. Economic burden of unintended pregnancy in the United States | RTI Health Solutions (rtihs.org)
25 Arora KS, Ponsaran R, Morello L, et al. Obstetrician–gynecologists’ practices in postpartum sterilization without a valid Medicaid consent form. Obstet Gynecol. 2021;138(1):66-72.
26 US Department of Health and Human Services. Immediate Office of the Secretary. HHS Regulations Toolkit. Last reviewed July 1, 2014. https://www.hhs.gov/regulations/regulations-toolkit/index.html