
In the ambulatory setting, women often present with breast and gynecologic concerns. These concerns are primarily the result of a benign condition. In the case of cancer, however, missing or delay in diagnosis due to time constraints, the need to maintain a patient schedule, or a provider’s perspective of a patient’s clinical presentation can ultimately contribute to the disproportionate mortality rates seen among minoritized women.1–3 During the Covid-19 pandemic, patients were significantly restricted from accessing health services. This disruption to health service access has resulted in an increase in patients presenting with advanced stages of cancer and has cast a light on the impact of social determinants of health (SDOH) that has been exacerbated due to the pandemic.4 Advanced practice registered nurses (APRNs) who provide women’s healthcare play a critical role in screening, early diagnosis, and treatment of breast and gynecologic cancers. As clinicians, we are committed to reducing disparities in morbidity and mortality that currently exist in the patient population in our care. This article provides an update on the current status of these disparities and discusses the role APRNs have in addressing SDOH and clinician bias to improve breast and gynecologic cancer outcomes.
Cancer disparities
Breast cancer is one of the most frequently diagnosed cancers among women in the United States. Improvements in diagnostic technologies and cancer therapeutics have contributed to substantial overall changes in reported breast cancer incidence and mortality. In 1975, 1 in 11 women were expected to be diagnosed with breast cancer over the course of their lifetime.5,6 This rate has changed to 1 in 8, a change attributable to improved screening guidelines and mammogram sensitivity.5,6 Although more breast cancers are being diagnosed, they are more likely to be early-stage tumors with correspondingly low rates of mortality. Unfortunately, mortality rates in minoritized women remain high. One cause for higher mortality in minoritized women is the increased incidence of triple-negative breast cancer (TNBC) among premenopausal, Hispanic, and non-Hispanic Black women.7,8 Due to the lack of targeted therapeutic options, 13% to 42% of women with TNBC have recurrence 19 to 40 months after treatment and the mortality rate is as high as 75% 3 months after the recurrence.9–12 Mortality among non-Hispanic Black women in the US remains the highest with 28 deaths per 100,000 women, followed by non-Hispanic White women (19.9) and American Indian/Alaska Native women (15.4) (Table).5,13
The American Cancer Society estimated the diagnosis of 14,100 new cases of cervical cancer and 4,280 deaths in 2022.9 Cervical cancer is most frequently diagnosed in women after age 30 years. Women over age 65 years still have a 20% chance of having cervical cancer due to access barriers to screening in addition to irregular screening history.14,15 Advances in cervical cancer screening with corresponding management of precancerous lesions have resulted in a downward trend in the incidence of cervical cancer, but disparities persist. American Indian and Alaska Native women have the highest cervical cancer incidence rate (10.9/100,000), followed by Hispanic women (9.7/100,000), but non-Hispanic Black women have the highest mortality rate compared with other racial and ethnic groups (3.4/100,000) (Table).13
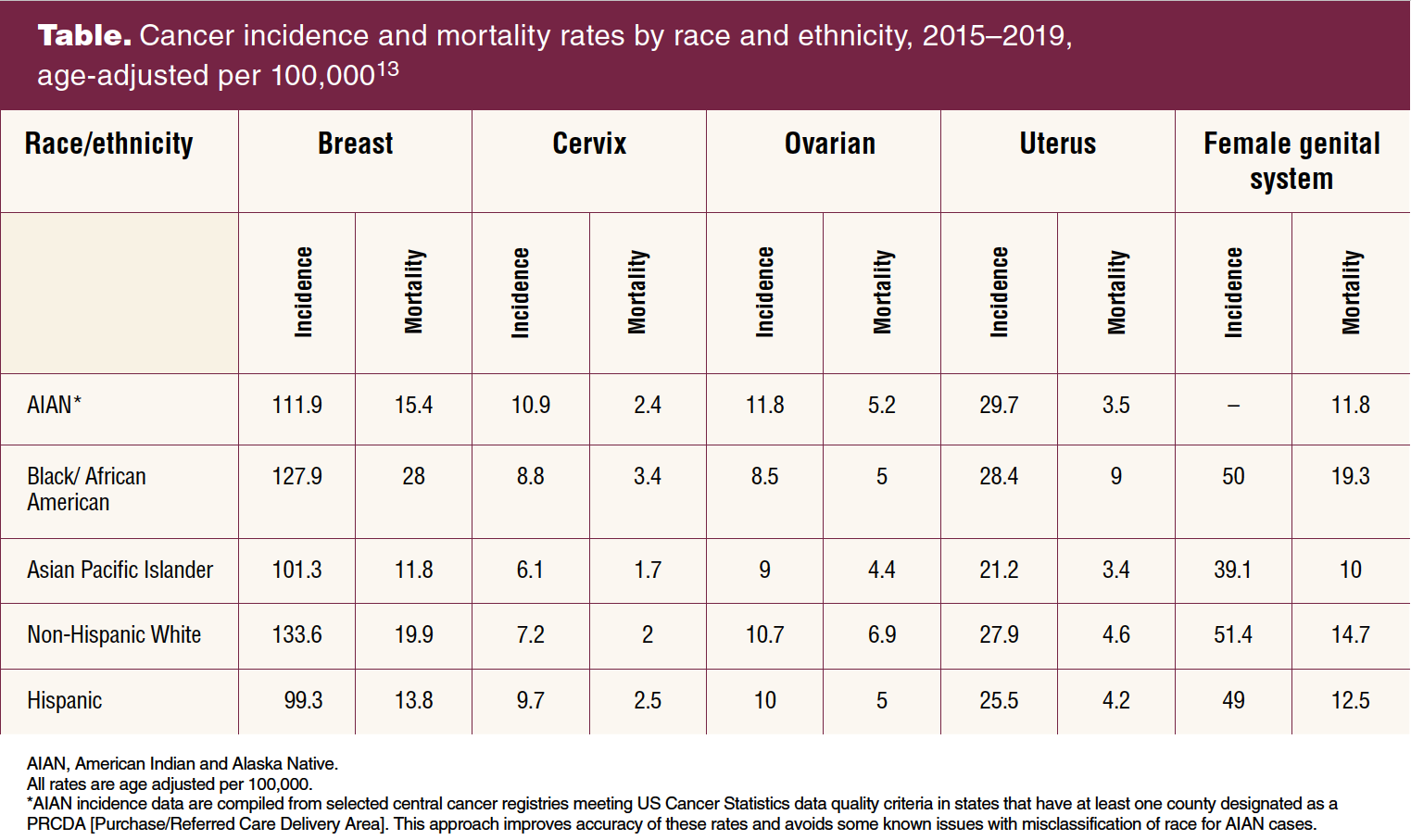
Unlike cervical cancer, there is no screening test for ovarian cancer. It is primarily diagnosed through a process of exclusion when signs and symptoms present (eg, abdominal bloating, abnormal uterine bleeding, quickly feeling full after eating, urinary frequency, back pain, dysuria, dyspareunia, pelvic pain). Mainly diagnosed in older women, ovarian cancer is the fifth leading cause of cancer mortality in women and the most deadly gynecologic cancer, with the highest incidence rates among women who are American Indian and Alaska Native (11.8/100,000) as compared to non-Hispanic White women (10.7/100,000) and non-Hispanic Black women (8.5/100,000).16 Non-Hispanic Black women have a lower ovarian cancer mortality rate (5/100,000) as compared to non Hispanic White women and American Indian and Alaska Native women (6.9/100,000 and 5.2/100,000, respectively) (Table).13 Of note, however, there has been an improvement in the relative 5-year survival rate for non-Hispanic White women with ovarian cancer, with an increase from 33% to 48% between 1975 and 2016, but for non-Hispanic Black women, there has been a decrease in the 5-year survival rate from 44% to 41% during the same time period.16
Similar to ovarian cancer, uterine cancer mainly affects postmenopausal women and there is no screening test. The mean age of diagnosis is 60 years.6 The presenting symptom is frequently abnormal uterine bleeding. The American Cancer Society estimates the highest incidence of uterine cancer is among American Indian and Alaska Native women followed by non-Hispanic Black women, whereas the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program reports the highest incidence to be among non-Hispanic Black women.6,17 Data from both organizations show that the highest mortality rates are experienced among non-Hispanic Black women (Table). 6,13,17
Addressing social determinants of health
Screening tests have proven to be effective in the early diagnosis and improved survival rates for breast cancer and cervical cancer. Screening tests for ovarian and uterine cancers could have the potential to decrease mortality rates but remain elusive. Even with highly sensitive screening tests, disparities in breast and cervical cancers for Hispanic, American Indian, Alaska Native, and non-Hispanic Black women largely persist due to the lack of access to screening services.18 Delays in treatment when diagnosis of breast or gynecologic cancer is made further contribute to disparities.
Reducing the structural barriers that contribute to breast and gynecologic cancer disparities requires a concerted effort by healthcare providers and healthcare systems. APRNs who provide women’s healthcare can improve cancer outcomes for minoritized women when they effectively address SDOH and learned, personal bias with each patient encounter.
It is clear that disparities in breast and gynecologic cancer incidence and mortality among non-Hispanic Black, American Indian, and Alaska Native women in the US persist. These cancer disparities have been attributed to SDOH that manifest as inequities in cancer risk and access to screening, diagnosis, and treatment. To address SDOH requires an understanding of the complex intersection of conditions in one’s environment that affect health. As early as 1899, the sociologist, historian, and civil rights activist W.E.B. DuBois described how social and physical environments are associated with chronic stress.19 Since the colonization of the US and continuing today, the dominant societal culture has exposed non-Hispanic Black and American Indian women to social and physical environments that create persistently high levels of stress. This chronic stress is a documented contributor to adverse health outcomes, including cancer development and progression.20–22 Chronic stress impairs the ability of the immune system to survey and aptly respond to tumorigenic signals in the cellular environment.22 Social scientists and cancer researchers alike are continuing to investigate the five SDOH: economic stability; education access and quality; neighborhood and built environment; social and community context; and healthcare access and quality, and their contribution to breast and gynecologic cancer disparities displayed on the national landscape.23
Systemic inequities in healthcare that prevent access for minoritized populations also result in disparities in cancer deaths.24 Barriers such as delayed referral to treatment, inadequate patient insurance, distance to care, provider bias, intergenerational trauma and related mistrust, high costs of care, communication and translation, and culturally incongruent care can result in disparate patient mortality.1–3,18 APRNs have the power to take action and decrease these barriers in the healthcare setting (Box).
Box. Recommendations for APRNs
- Learn the barriers that obstruct access to women’s healthcare in the community that you serve.
- Make a list of community cancer and health resources available for your patients in the community in which they live.
- Be aware of how your bias can delay cancer diagnosis, treatment, and increase patient suffering and ultimately, patient mortality.
- Create a diverse and culturally aware clinical space through staffing, patient literature, and environmental cues.
- Stay engaged in working with stakeholders at the local and national level to remove barriers that prevent access to care for women with breast and gynecologic cancers.
- Encourage stakeholders to financially support the development of highly sensitive screening tests for ovarian and uterine cancer.
- Ensure availability of certified interpreters for all patient populations you serve, including Indigenous languages.
- Speak with patients about the barriers they experience in accessing care, being mindful of structural conditions that drive barriers such as access to education, infrastructure and built environment, economic stability, and social and community context.
It is critical to learn about the barriers that obstruct access to women’s healthcare in the community you serve. Talk with patients about the barriers they experience in accessing care. Be mindful of structural conditions that drive barriers such as access to education, infrastructure and built environment, economic stability, and social and community context. Identify culturally congruent community resources for cancer care, financial assistance, transportation, nutrition, and other needed support that you can share with patients.25 Advocate for action at local and national levels to remove barriers that prevent access to care for women at risk for or with breast and gynecologic cancers.
It is important to take a close look at your clinical setting. Create a diverse and culturally aware clinical space through staffing, patient literature, and environmental cues. Intentionally diversify staff from the front desk to clinicians to match with the diversity in your community and patient population.26 Be aware that information and education communicated in a way that hinders a patient’s ability to understand a cancer diagnosis can contribute to an inability to actively engage in their care, ultimately widening cancer disparities.27 Educational leveling (eg, literacy level, language options, materials with images/demonstrations) is one approach that can reduce barriers to understanding. Ensure availability of certified interpreters for all patient populations you serve, including Indigenous languages. These steps can aid in circumventing barriers that can arise due to cross-cultural miscommunication.26
Research and its translation into evidence-based practice is critical to reduce disparities in breast and gynecologic cancer incidence and mortality. APRNs can lead and participate in studies that explore best practices in clinical and community settings to reduce barriers created by SDOH, increasing access to cancer risk reduction, screening, early diagnosis, and treatment. They have a significant role in translating evidence to practice in the clinical and community setting to reduce disparities in care and improve cancer-related outcomes. Outside of their own clinical setting, APRNs can make an effort to stay aware of clinical trials open for patient participation and refer patients for inclusion, thereby helping to create a more robust patient cohort or available archival samples to provide more generalizable data to the national patient landscape.28 As well-informed advocates, they can effect health policy and funding to support research leading to improved screening technologies for all breast and gynecologic cancers, better diagnostic tools, and more effective treatments that can be equitably distributed.
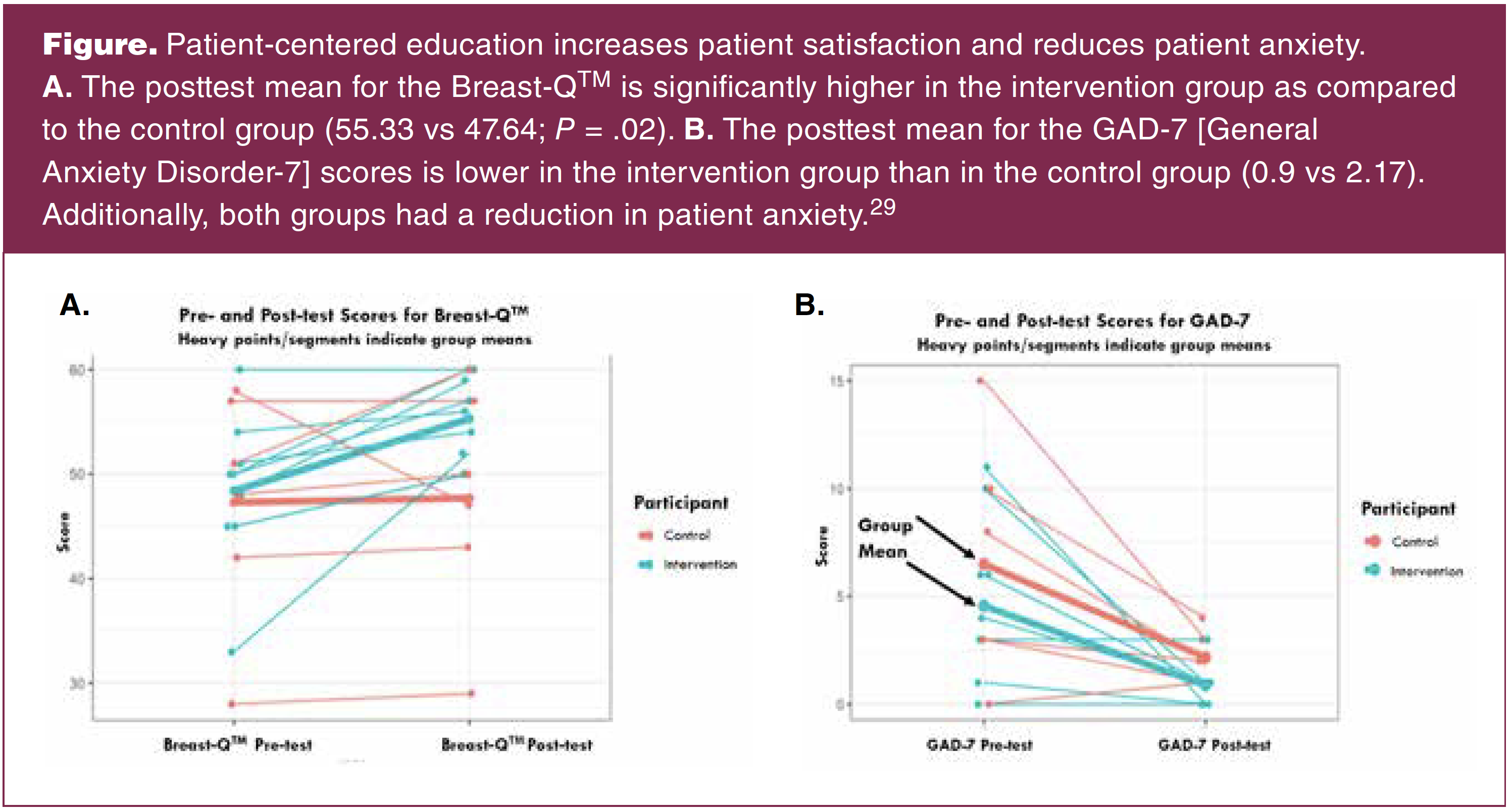
Evidence-based interventions implemented by doctor of nursing practice-prepared APRNs are on the rise in clinical practice. Patient education that engages a patient so that they clearly understand their diagnosis and plan of care not only improves patient outcomes but also levels the SDOH of education access and quality. For example, a patient-centered intervention was developed to reduce patient anxiety and improve patient understanding in women diagnosed with breast cancer and undergoing breast reconstruction. This intervention was led by an APRN who educated breast cancer patients about their procedure using culturally appropriate materials and a teach-back mannequin. Data from this cohort study consisting largely of Hispanic women (71%) demonstrate that this patient-centered intervention increased patient satisfaction (Figure. A; P > .02), as measured by Breast-Q™, and decreased patient anxiety (Figure. B) as compared to educational materials alone, indicating that interventions centered on patient understanding and feedback positively influence patient satisfaction.29 This evidence-based strategy can be modified to meet the needs of other minoritized groups through the modification and translation of teaching materials and thoughtful implementation with a knowledgeable interventionist.
Addressing implicit bias
Implicit bias, the learned stereotypes and prejudices that automatically and unconsciously influence behavior can unintentionally impact a healthcare provider’s relationship with patients and colleagues.30
Implicit bias affects patient–clinician interactions, diagnostic and treatment decisions, patient adherence to health-related recommendations, and ultimately patient outcomes.3,18,24,30,31 Women’s healthcare providers can improve cancer outcomes for patients when they attend to their own assumptions and implicit biases. Although many people would believe their clinical practice is objective and without prejudice, recent research has established that clinicians who have made deliberate efforts and developed an awareness of their implicit biases improved clinical care in multiple domains.32,33 A first step can be to explore and identify one’s own stereotypes and prejudices by taking implicit association tests or through other means of self-analysis. Project Implicit provides a variety of implicit association tests with analysis (implicit.harvard.edu/implicit/). Being aware of one’s implicit biases allows the healthcare provider to implement intentional strategies that increase their ability to be present to “hear” each patient as they describe their health concerns and communicate to others in an unbiased manner, improving care for that patient across systems.
Conclusion
Disparities in breast and gynecologic cancers persist for non-Hispanic Black, Hispanic, American Indian, and Alaska Native women. But pivots such as provider introspection, diversification of clinical providers and staff, reduction of barriers to healthcare access, and intentional engagement of APRNs in the implementation of evidence-based practice in clinical care to address SDOH can ultimately reduce cancer disparities. The responsibility of APRNs providing women’s healthcare is to be aware and brave enough to make the pivots that will result in changes both in individual practice and the removal of system barriers that prevent access to women who disproportionately experience high mortality due to breast and gynecologic cancer.
Tamala Murray is breast oncology advanced practice registered nurse at Harbor-UCLA in Torrance, California. Emily Haozous is a research scientist at the Pacific Institute for Research and Evaluation in Albuquerque, New Mexico. Su Yon Jung is Associate Professor, Eden Brauer is Assistant Professor, Catherine Carpenter is Adjunct Professor, and Nalo M. Hamilton is Associate Professor at the UCLA School of Nursing in Los Angeles, California. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(5):21-26. doi: 10.51256/WHC102321
References
1 Basu A, Ghosh D, Mandal B, et al. Barriers and explanatory mechanisms in diagnostic delay in four cancers – A health-care disparity? South Asian J Cancer. 2019;8(4):221-225.
2 Hanna TP, King WD, Thibodeau S, et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020;371:m4087.
3 Dolly D, Mihai A, Rimel BJ, et al. A delay from diagnosis to treatment is associated with a decreased overall survival for patients with endometrial cancer. Front Oncol. 2016;6:31.
4 Rucinska M, Nawrocki S. COVID-19 pandemic: impact on cancer patients. Int J Environ Res Public Health. 2022;19(19):12470.
5 National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Female breast cancer. https://seer.cancer.gov/statfacts/html/breast.html.
6 National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Cancer Statistics Explorer Network. Uterine cancer. https://seer.cancer.gov/statistics-network/.
7 Bauer KR, Brown M, Cress RD, et al. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer registry. Cancer. 2007;109(9):1721-1728.
8 Prakash O, Hossain F, Danos D, et al. Racial disparities in triple negative breast cancer: a review of the role of biologic and non-biologic factors. Front Public Health. 2020;8:576964.
9 Yin L, Duan JJ, Bian XW, Yu SC. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020;22(1):61.
10 Gluz O, Liedtke C, Gottschalk N, et al. Triple-negative breast cancer—current status and future directions. Ann Oncol. 2009;20(12):1913-1927.
11 Steward L, Conant L, Gao F, Margenthaler JA. Predictive factors and patterns of recurrence in patients with triple negative breast cancer. Ann Surg Oncol. 2014;21(7):2165-2171.
12 Stewart RL, Updike KL, Factor RE, et al. A multigene assay determines risk of recurrence in patients with triple-negative breast cancer. Cancer Res. 2019;79(13):3466-3478.
13 Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33.
14 American Cancer Society. Cancer Statistics Center: Cervix. 2023. https://cancerstatisticscenter.cancer.org/#!/cancer-site/Cervix.
15 Zeno EE, Brewer NT, Spees LP, et al. Racial and ethnic differences in cervical cancer screening barriers and intentions: the My Body My Test-3 HPV self-collection trial among under-screened, low-income women. PLoS ONE. 2022;17(10):e0274974.
16 American Cancer Society. Cancer Statistics Center: Ovary. 2023. https://cancerstatisticscenter.cancer.org/#!/cancer-site/Ovary.
17 American Cancer Society. Key Statistics for Endometrial Cancer. 2023. https://www.cancer.org/cancer/types/endometrial-cancer/about/key-statistics.html.
18 Caraballo C, Ndumele CD, Roy B, et al. Trends in racial and ethnic disparities in barriers to timely medical care among adults in the US, 1999 to 2018. JAMA Health Forum. 2022;3(10):e223856.
19 Du Bois WEB. The Philadelphia Negro: A Social Study. New York: Schocken Books; 1899, 1967.
20 Woods-Giscombe CL. Superwoman schema: African American women’s views on stress, strength, and health. Qual Health Res. 2010;20(5):668-683.
21 Palacios JF, Portillo CJ. Understanding Native women’s health: historical legacies. J Transcult Nurs. 2009;20(1):15-27.
22 Zenga J, Awan MJ, Frei A, et al. Chronic stress promotes an immunologic inflammatory state and head and neck cancer growth in a humanized murine model. Head Neck. 2022;44(6):1324-1334.
23 US Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Healthy People 2030. Social De-terminants of Health. https://health.gov/healthypeople/priority-areas/social-determinants-health.
24 Brown AF, Ma GX, Miranda J, et al. Structural interventions to reduce and eliminate health disparities. Am J Public Health. 2019;109(S1):S72-S78.
25 Alexis AC. Cultural competence in nutrition and dietetics: what we need to know. Healthline. April 9, 2021. https://www.healthline.com/nutrition/cultural-competence-in-dietetics.
26 Jones RA, Hirschey R, Campbell G, et al. Update to 2019-2022 ONS research agenda: rapid review to address structural racism and health inequities. Oncol Nurs Forum. 2021;48(6):589-600.
27 Foster J, Idossa L, Mau LW, Murphy E. Applying health literacy principles: strategies and tools to develop easy-to-read patient educa-tion resources. Clin J Oncol Nurs. 2016;20(4):433-436.
28 Cohn EG, Hamilton N, Larson EL, Williams JK. Self-reported race and ethnicity of US biobank participants compared to the US census. J Community Genet. 2017;8(3):229-238.
29 Mundy LR, Homa K, Klassen AF, et al. Breast cancer and reconstruction: normative data for interpreting the BREAST-Q. Plast Reconstr Surg. 2017;139(5):1046e-1055e.
30 National Association of Nurse Practitioners in Women’s Health. Position Statement. Structural Racism and Implicit Bias in Women’s Healthcare. Womens Healthcare. 2020;8(6):13-16.
31 Williams DR, Lawrence JA, Davis BA, Vu C. Understanding how discrimination can affect health. Health Serv Res. 2019;54(suppl 2):1374-1388.
32 Nolan TS, Alston A, Choto R, Moss KO. Cultural humility: retraining and retooling nurses to provide equitable cancer care. Clin J Oncol Nurs. 2021;25(5):3-9.
33 Edgoose JYC, Quiogue M, Sidhar K. How to identify, understand and unlearn implicit bias in patient care. Fam Pract Manag. 2019;26(4):29-33
KEY WORDS: breast cancer, social determinants of health, gyn cancers, patient-centered education, health disparities