
The National Association of Nurse Practitioners in Women’s Health (NPWH), along with numerous other national health professional organizations, affirms that abortion is an essential component of comprehensive reproductive healthcare and that it should be legal, safe, and accessible.1–10 Legal restrictions do not eliminate abortion but instead increase the likelihood that abortions will be performed unsafely, with the potential for complications and death.11 Legislative and policy decisions should be firmly rooted in science, protect the patient–clinician relationship, and aim at reducing disparities to ensure equitable access to safe, effective, and timely abortion care.
People with low incomes, those living in rural areas, people from racial and ethnic minority groups, adolescents, individuals who are incarcerated, transgender men, immigrants, and others who are marginalized are disproportionately affected by barriers to and restrictions on abortion access.2,5,12–17 NPWH advocates for policies and evidence-based initiatives that promote equity and reduce disparities in all aspects of reproductive health including abortion care.18 NPWH supports a reproductive justice framework based on three core principles: the right to have children, not have children, and parent children in safe and sustainable communities.19
NPWH’s mission includes “protecting and promoting a woman’s right to make her own choices regarding her health and wellbeing within the context of her lived experience and her personal, religious, cultural, and family beliefs.”20 NPWH recognizes that some people who do not identify as women are able to become pregnant, and transgender people, gender nonconforming people, and people of diverse gender identities are also affected by abortion restrictions. NPWH asserts that reproductive healthcare must be comprehensive, accessible, safe, and inclusive for all individuals. NPWH supports the right of individuals to have access to factual, evidence-based information to make their own informed reproductive choices.
Background
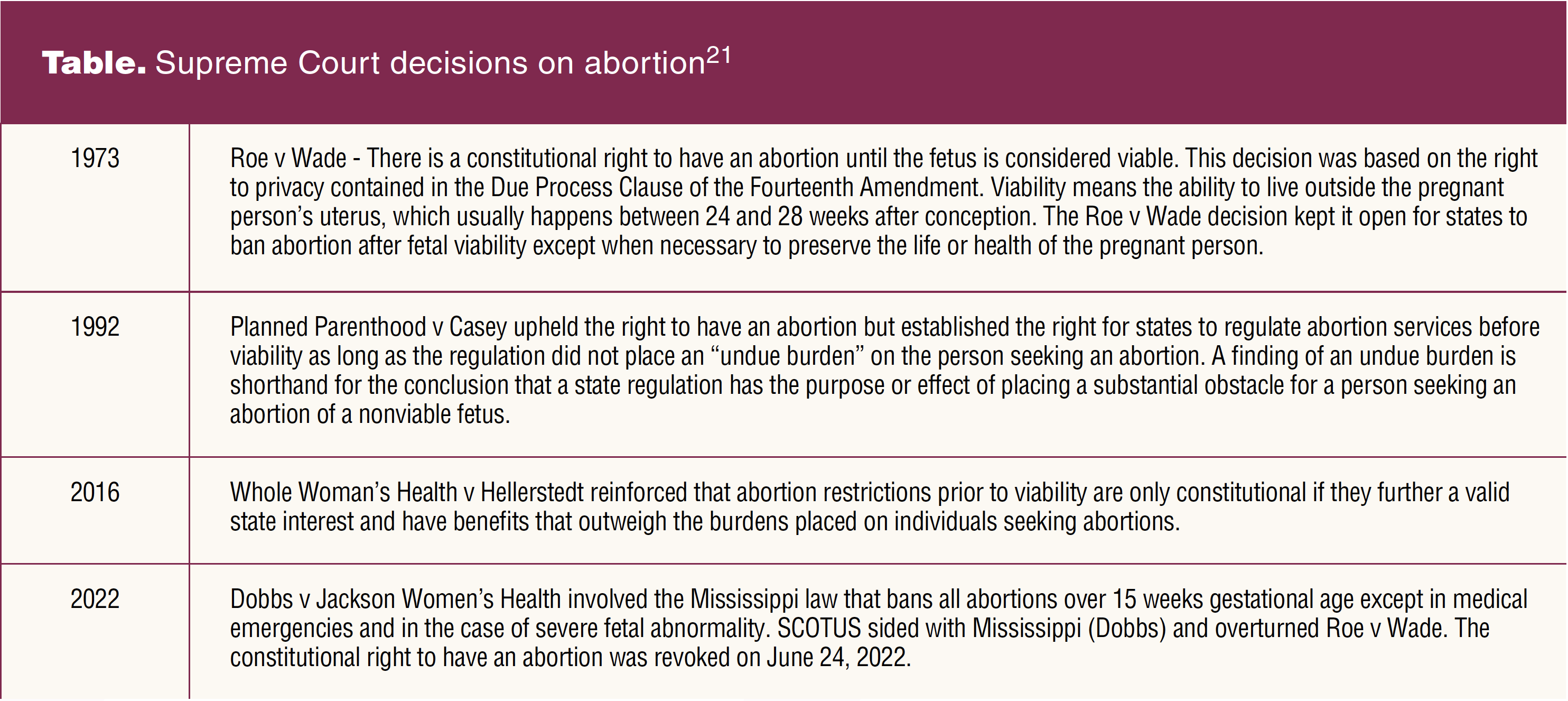
On June 24, 2022, the Supreme Court of the United States (SCOTUS) overturned Roe v Wade, thus abandoning the constitutional right to have an abortion that had been in place for almost 50 years. The history of legislation in the US regarding the right to have an abortion and the right to provide abortion services is relevant for understanding the current legislative and political environment. See the Table for Supreme Court decisions on abortion.21
The SCOTUS ruling overturning Roe v Wade allows each state to enact its own laws that support, restrict, or ban abortion. At the time of this ruling, over half of the states in our country are poised to enact restrictive laws. Current and potential state legislative restrictions target individuals seeking abortion and healthcare clinicians who provide abortion services or counsel patients about such services. States have or are expected to place bans on abortion at arbitrary gestational ages and to mandate scripted counseling, ultrasounds, waiting periods, and parental involvement. In addition, states have or are expected to place restrictions on providing medication abortion and to implement obstructive abortion facility and staffing requirements. None of these restrictions is based on scientific evidence pertaining to the safety of abortion. Rather, such restrictions delay and limit access to services at a reasonable distance from home, increase the cost of care, interfere with the patient–clinician relationship, and compromise quality.
The environment in many states is hostile to clinicians who provide abortion services. The looming threat of criminalizing the provision of abortions, the stigma and threats of violence clinicians who provide abortions may face in their own communities, and the lack of available training in states that ban abortion contribute to a reduction in the number of abortion care facilities and skilled providers.5,12,22
Abortion procedures are safe. From 2013 to 2018, the national fatality rate for legally induced abortion was 0.41 deaths per 100,000 abortions.23 The complication rate is estimated to be 2.1%, with most (1.87%) of these considered minor such as pain, bleeding, mild infection, and post-anesthesia complications.24 The risk of death associated with childbirth is approximately 14 times higher than that with abortion.25 Evidence indicates that medication abortion provided in person or via telehealth is safe and effective and has a high degree of patient satisfaction.26–28
A National Academies of Sciences Engineering and Medicine (NASEM) committee reviewed the state of the science on all methods of abortion and published a document on the safety and quality of abortion care in the US in 2018. This document affirms that abortion is safe and that it is unnecessary and burdensome regulations that threaten the quality of abortion care.29 In countries where abortion is illegal or not readily accessible, the numbers of abortions do not decline. Instead, people resort to unsafe abortion attempts resulting in a range of complications and death.30–31
When assessing the safety of any medical procedure, it is important to consider both short-term safety and potential long-term health consequences. Through a review of high-quality research, the NASEM committee determined that having an abortion does not increase the risk for secondary infertility, pregnancy-related hypertensive disorders, abnormal placentation, preterm birth, breast cancer, or mental health disorders (ie, depression, anxiety, post-traumatic stress disorder).29
On the other hand, there is evidence that denying access to a desired abortion can result in long-term socioeconomic consequences. The Turnaway study followed 813 participants for 5 years after they were either prevented from obtaining a wanted abortion because of gestational age limits or able to obtain an abortion. The majority of the women in the study, whether or not they were able to obtain an abortion, were living in poverty at baseline. Women in this study who were turned away and went on to give birth were more likely to have an increase in household poverty that lasted at least 4 years, reductions in full-time employment, greater reliance on public assistance, and were more likely to raise children alone.32
Despite considerable evidence supporting the safety of abortion in the US and the lack of long-term negative consequences for physical or mental health, misinformation about abortion continues to be presented in state-mandated informed consent scripts, in abstinence-only education programs, at crisis pregnancy centers, and from internet sources.33,34 Misinformation hinders informed decision making among those considering their pregnancy options.
Implications for women’s healthcare providers
Patients look to healthcare providers as trusted sources of information and advocates for quality healthcare. As healthcare providers, we honor all people’s rights to self-determination, autonomy, privacy, and respect. As we face uncertainty about abortion access, it is essential for healthcare providers to be able to provide patients who desire abortion with accurate information about regulations at the federal level and within the state in which they reside, as well as what safe and legal options exist for them. Efficient and effective referral systems are important to have in place to connect patients with safe and timely abortion care.35 The Box includes resources available to support evidence-based conversations with people about all pregnancy options and current federal and state regulations.
Box. Resources
| Abortion Finder. State-by-State Guide abortionfinder.org/abortion-guides-by-state ACOG Guide to Language and Abortion acog.org/contact/media-center/abortion-language-guide Advancing New Standards in Reproductive Health ansirh.org CDCs Abortion Surveillance System FAQs cdc.gov/reproductivehealth/data_stats/abortion.htm Center for Reproductive Rights reproductiverights.org Guttmacher Institute. State Policies on Abortion guttmacher.org/united-states/abortion/state-policies-abortion National Abortion Federation Clinical Policy Guidelines for Abortion Care (2022) prochoice.org/wp-content/uploads/2022-CPGs.pdf NPWH. Reproductive Rights Policy Summary cdn.ymaws.com/npwh.org/resource/resmgr/positionstatement/npwh_reproductive_rights_pol.pdf Planned Parenthood. Abortion Clinics Near You plannedparenthood.org/abortion-access |
NPWH respects the right of healthcare providers to determine their personal viewpoints related to abortion. NPWH also respects the right of every pregnant person to have access to accurate and unbiased information on abortion as a pregnancy option. It is imperative that the pregnant person is able to obtain this information in a timely manner that does not impede informed decision making and access to abortion if desired.
NPWH leadership
NPWH will provide leadership to ensure:
- Women’s health nurse practitioners (WHNPs) and other advanced practice clinicians have access to continuing education programs and other resources for evidence-based information on abortion and on pregnancy options counseling.
- WHNP educational programs have access to evidence-based information on abortion and on pregnancy options counseling that can be incorporated into curricula.
- Collaborative engagement with other health professional organizations to advocate for access to abortion, as well as the full scope of reproductive healthcare, and policies that support initiatives to address inequities in all aspects of reproductive health.
- Research moves forward to promote best practices for access to high-quality abortion care.
References
1 American Academy of Family Physicians. Resolution No. 412 (New York C) – Affirming the Safety and Legality of Abortion. 2019. www.reproductiveaccess.org/wp-content/uploads/2020/01/Resolution-No.-412-New-York-C-affim…y-of-Abortion-Congress-of-Delegates-2019.pdf.
2 American Academy on Adolescence. The adolescent’s right to confidential care when considering abortion. Pediatrics. 2017;139(2):e20163861.
3 American College of Nurse-Midwives. Position statement. Access to comprehensive sexual and reproductive health care services. 2016. https://www.midwife.org/acnm/files/ACNMLibraryData/UPLOADFILENAME/000000000087/Access-to-Comprehensive-Sexual-and-Reproductive-Health-Care-Services-FINAL-04-12-17.pdf.
4 American College of Obstetricians and Gynecologists. Abortion policy. Statement of policy. 2022. https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/abortion-policy.
5 American College of Obstetricians and Gynecologists. Increasing access to abortion. Committee opinion no. 815. Obstet Gynecol. 2020;136(6):e107-e115.
6 Supreme Court of the United States. Amicus Brief. Dobbs et al, petitioners v Jackson Women’s Health Organization, et al, respondents. September 20, 2021. https://www.supremecourt.gov/DocketPDF/19/19-1392/192909/20210920125441954_19-1392%20Thomas%20E%20Dobbs%20v%20Jackson%20Womens%20Health%20Brief%20of%20Amici%20in%20Support.._.pdf.
7 American Psychological Association. APA Resolution Affirming and Building on APA’s History of Support for Reproductive Rights. February 2022. www.apa.org/about/policy/resolution-reproductive-rights.pdf.
8 Association of Women’s Health, Obstetric and Neonatal Nurses. AWHONN position statement: Health care decision making for reproductive care. J Obstet Gynecol Neonatal Nurs. 2016;45(5):718.
9 Espey E, Dennis A, Landy U. The importance of access to comprehensive reproductive health care, including abortion: a statement from women’s health professional organizations. Am J Obstet Gynecol. 2019;220(1):67-70.
10 Society for Maternal-Fetal Medicine. Access to Abortion Services. An Official Position Statement of the Society for Maternal-Fetal Medicine. June 2020. https://s3.amazonaws.com/cdn.smfm.org/media/2418/Access_to_Abortion_Services_(2020).pdf.
11 Fathalla MF. Safe abortion: the public health rationale. Best Pract Res Clin Obstet Gynaecol. 2020;63:2-12.
12 Anderson EM, Cowan SK, Higgins JA, et al. Willing but unable: physicians’ referral knowledge as barriers to abortion care. SSM Popul Health. 2022;17:101002.
13 Fuentes L, Jerman J. Distance traveled to obtain clinical abortion care in the United States and reasons for clinic choice. J Womens Health. 2019;28(12):1623-1631.
14 Knittel A, Ti A, Schear S, Comfort M. Evidence-based recommendations to improve reproductive healthcare for incarcerated women. Int J Prison Health. 2017;13(3-4):200-206.
15 Light A, Wang L-F, Zeymo A, Gomez-Lobo V. Family planning and contraception use in transgender men. Contraception. 2018;98(4):266-269.
16 Messing AJ, Fabi RE, Rosen JD. Reproductive injustice at the US border. Am J Public Health. 2020;110(3):339-344.
17 Sutton MY, Anachebe NF, Lee R, Skanes H. Racial and ethnic disparities in reproductive health services and outcomes, 2020. Obstet Gynecol. 2021;137(2):225-233.
18 National Association of Nurse Practitioners in Women’s Health. Reproductive Rights Policy Summary. May 2022. https://cdn.ymaws.com/npwh.org/resource/resmgr/positionstatement/npwh_reproductive_rights_pol.pdf.
19 Sister Song. Reproductive justice. http://sistersong.net/reproductive-justice/. June 16, 2022.
20 National Association of Nurse Practitioners in Women’s Health. About NPWH. Our mission. https://npwh.org/page/about-npwh.
21 Sobel L, Ramaswamy A, Salganicoff A. Abortion at SCOTUS: Dobbs v. Jackson Women’s Health. Kaiser Family Foundation Issue Brief. May 4, 2022. https://www.kff.org/womens-health-policy/issue-brief/abortion-at-scotus-dobbs-v-jackson-womens-health/.
22 Vinekar K, Karlapudi A, Nathan L, et al. Projected implications of overturning Roe v Wade on abortion training in U.S. obstetrics and gynecology residency programs. Obstet Gynecol. 2022;00(00):1-4.
23 Kortsmit K, Mandel MG, Reeves JA, et al. Abortion surveillance – United States, 2019. MMWR Surveill Summ. 2021;70(9):1-29.
24 Upadhyay UD, Desai S, Zlidar V, et al. Incidence of emergency department visits and complications after abortion. Obstet Gynecol. 2015;125(1):175-183.
25 Raymond EG, Grimes DA. The comparative safety of legal induced abortion and childbirth in the United States. Obstet Gynecol. 2012;119(2 Pt 1):215-219.
26 Aiken ARA, Lohr PA, Lord J, et al. Effectiveness, safety, and acceptability of no-test medical abortion (termination of pregnancy) provided via telemedicine: a national cohort study. BJOG. 2021;128(9):1464-1474.
27 Grossman D, Grindlay K. Safety of medical abortion provided through telemedicine compared with in person. Obstet Gynecol. 2017;130(4):778-782.
28 Upadhyay UD, Raymond EG, Koenig LR, et al. Outcomes and safety of history-based screening for medication abortion: a retrospective multicenter cohort study. JAMA Intern Med. 2022;182(5):482-491.
29 National Academies of Sciences, Engineering, and Medicine. The Safety and Quality of Abortion Care in the United States. Washington, DC: National Academies Press, 2018.
30 Akinlusi FM, Rabiu KA, Adewunmi AA, et al. Complicated unsafe abortion in a Nigerian teaching hospital: pattern of morbidity and mortality. J Obstet Gynaecol. 2018;38(7):961-966.
31 Yokoe R, Rowe R, Choudhury SS, et al. Unsafe abortion and abortion-related death among 1.8 million women in India. BMJ Glob Health. 2019;4(3):e001491.
32 Foster DG, Biggs MA, Ralph L. Socioeconomic outcomes of women who receive and women who are denied wanted abortions in the United States. Am J Public Health. 2018;108(3):407-413.
33 Berglas NF, Gould H, Turok DK. State-mandated (mis)information and women’s endorsement of common abortion myths. Womens Health Issues. 2017;27(2):129-135.
34 Patey AJ, Hood KB. Towards a better understanding of abortion misinformation in the USA: a review of the literature. Cult Health Sex. 2021;23(3):285-300.
35 Verma N, Shainker SA. Maternal mortality, abortion access, and optimizing care in an increasingly restrictive United States: a review of the current climate. Semin Perinatol. 2020;44(5):151269.
NPWH gratefully acknowledges Caroline Hewitt, DNS, WHNP-BC, ANP-BC; Mary Hickey, EdD, WHNP-BC, FNP-BC; Beth Kelsey, EdD, APRN, WHNP-BC; Amy Levi, PhD, CNM, WHNP-BC; Shawana Moore, DNP, APRN, WHNP-BC; Lisa Stern, MSN, WHNP-BC, ANP-BC; and Jacki Witt, JD, MSN, WHNP-BC, for their contributions as writing group members of this position statement.
Approved by NPWH Board of Directors: August 15, 2022