
The National Association of Nurse Practitioners in Women’s Health (NPWH) affirms the right of each individual or couple who desire to use contraception to be able to do so. Barriers to obtaining and successfully using contraception must be eliminated, particularly for the most vulnerable individuals and populations. NPWH advocates for federal- and state-level policies that remove barriers and increase access to affordable, safe, and effective contraceptive methods for all reproductive-aged individuals. Multiple strategies involving legislation, regulations, consumer education, and innovation are necessary. Over-the-counter (OTC) access to hormonal contraceptives (HCs) and pharmacist-provided HCs are two specific strategies that can lower barriers to obtaining safe, effective contraception.
NPWH will provide leadership through policy advocacy, consumer and healthcare provider (HCP) education, and support of research on outcomes related to innovative strategies to expand access to HCs. NPWH supports the right of all individuals to access comprehensive sexual and reproductive health services and to make choices that meet their own needs.
Background
The concepts of desiring/not desiring a pregnancy and intended/unintended pregnancy are complex, especially when ambivalence about pregnancy, power inequities in relationships, family pressures, belief that one cannot become pregnant, and cultural and religious norms are taken into account. However, for purposes of data collection and analysis in demography and public health studies, the term unintended pregnancy is defined as pregnancy that is mistimed or unwanted.1 Although unintended pregnancy rates declined overall from 51% in 2008 to 45% in 2011,2 disparities persist. Unintended pregnancy rates are highest among women who are poor and/or low-income, members of minorities, younger than 25 years, less educated, and/or cohabiting with their sexual partner.2 Approximately 60% of women with unintended pregnancies were not using contraception during the month that they became pregnant.3
Reproductive-aged, sexually active individuals who do not want to become pregnant but who do not use effective contraception off er a variety of reasons for not doing so. Some of the reasons cited for not using HCs in particular include lack of access to and/or inconveniences associated with healthcare appointments needed to obtain prescriptions for HCs, the assumption that a pelvic examination is required to obtain HCs, the high cost, and concerns about safety and side effects.3-6 In addition, adolescents’ concerns about confidentiality may deter them from seeking highly effective contraceptive methods.3-7 OTC access to HCs and pharmacist-provided HCs might eliminate some, albeit not all, of these barriers.
Establishing OTC access to HCs requires action at the federal level through the FDA. When a company submits an application to the FDA to change the status of a product from prescription to OTC, reviewers of the application determine whether the medication has an established high safety profile and low potential for misuse or abuse, and whether labeling exists or could be developed so that consumers would be able to use the medication safely, without HCP intervention.8 To date, only one company, based in France, has initiated an FDA application to change its HC product, a progestin-only pill (POP), from prescription to OTC status.9 This process may be streamlined because the FDA has already approved OTC status for emergency-contraceptive POPs and because POPs have few contraindications. Nevertheless, the process is still complex and may take up to 3-4 years to complete.9 In addition, major concerns persist regarding the potential for federal regulatory policies to limit HC access for adolescents or to fail to guarantee insurance coverage for OTC HCs.10 Expanding access at the state level, although still posing some restrictive challenges, has thus far proved less time consuming and less cumbersome than going through the relabeling process with the FDA.
As of 2016, 47 states and the District of Columbia (DC) have statutes allowing creation of collaborative practice agreements (CPAs) for qualified pharmacists, which enable them to initiate, modify, and/or discontinue drug therapy for a variety of conditions. A CPA for this purpose is an agreement between a pharmacist and one or more prescribing HCPs that permits the pharmacist to work within the context of a defined protocol and assume professional responsibility for certain aspects of medication management. Although statutory language and additional requirements such as training and continuing education vary from state to state, none include restrictions about which specific health conditions approved CPAs may address. Therefore, use of CPAs for pharmacist provision of HCs is a possibility in each of these states and DC.11
To date, 12 states and DC have passed or proposed legislation to expand access to HCs through pharmacist provision—without the prospective HC user being required to be seen first by an HCP to obtain a prescription.12 Types of HCs (e.g., oral, transdermal, vaginal ring, injection), age restrictions, training requirements, specifics of protocols, and insurance coverage vary from state to state.12,13
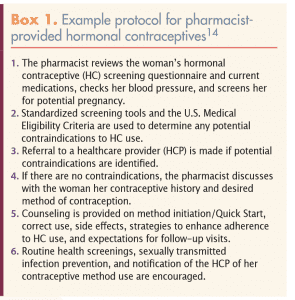
The establishment of CPAs, standing orders, or other types of written agreements, along with training and the use of standardized protocols to screen for contraindications/risks and provide education about a chosen HC method, allow pharmacists to provide HCs safely. Box 1 presents an example protocol.14 For persons without pre-existing risk factors or conditions, the overall health risk of using HCs is very low.15,16 Studies have found that women are able to self-screen reliably for these pre-existing risk factors or conditions.17-19 A study in Washington State supported pharmacists’ ability to identify individuals with/ without contraindications to HCs by using a screening checklist and measuring blood pressure.20
Pharmacist provision of HCs offers the advantages of convenient locations, extended hours of operation, and walk-in access without appointments. However, for this service to succeed, several potential barriers must be addressed. Barriers for pharmacists include the time required for training, already demanding workloads, and, most notably, lack of insurance reimbursement for time spent on assessment and counseling. Legislation in some states has addressed the lattermost barrier by expanding pharmacists’ scope of practice to enable direct billing for time spent providing the service.21 For individuals desiring contraceptives, a major barrier involves lack of knowledge about the availability of pharmacist-provided HCs—a service that would obviate the need for a prior HCP visit and prescription in most cases. Individuals without insurance that covers HCs may not be able to afford the fee for the pharmacist’s time and the cost of the HCs. Still, several studies indicate that most women at risk for unintended pregnancy believe HCs should be available without prescription and would use pharmacy access themselves.22-25
In 2016, NPWH signed onto a statement of purpose published by the Oral Contraceptives (OCs) OTC Working Group, a coalition of reproductive health, rights, and justice organizations; nonprofit research and advocacy groups; university-based researchers; and prominent clinicians committed to providing easier access to safe, effective, acceptable, and affordable contraceptives to all reproductive-aged individuals.26 The Working Group focuses on the potential to reduce disparities in reproductive healthcare access and outcomes among low-income, poor, and young women through OTC access to OCs. Activities of the group include engaging in public education and discussion, building consensus on key issues, and conducting research to maximize benefits and minimize risks regarding OTC OCs. The Working Group supports policies that expand coverage of OTC OCs in all public and private insurance plans and that ensure adolescents have full access to OTC contraceptives. Other professional HCP organizations that have signed on to the statement are listed in Box 2.26
Implications for women’s healthcare and WHNP practice
WHNPs are experts in helping individuals and couples choose and use contraceptive methods that are safe and effective and that meet their personal needs and preferences. As such, WHNPs should be in the forefront of designing, implementing, and evaluating new models of care to increase access to safe and effective contraception. WHNPs can seek out opportunities to lead in terms of writing protocols, creating self-screening forms, and developing education materials that can be used by pharmacists when providing HCs. Legislators need to hear from all NPs who practice evidence-based reproductive healthcare and who have witnessed the impact of disparities in access to contraceptives.
Over-the-counter or pharmacist-provided HCs cannot address all barriers to access and use of safe and effective contraceptives. In states with age restrictions for OTC/ pharmacist-provided HCs, persons younger than the minimum allowable age will still not be able to gain access to them. Individuals whose health insurance does not cover OTC or pharmacist-provided HCs may not be able to afford them. Finally, expanded access to HCs, either through OTC availability or through pharmacist provision of them, does not pertain to highly effective long-acting reversible contraceptive methods that may be desired—because these methods require an HCP visit.
Regardless of whether they can obtain HCs without a prescription, many individuals will continue to seek sexual and reproductive healthcare. NPs who provide this care must continue to fi nd ways to make it accessible, affordable, and acceptable for everyone and to address the needs of vulnerable populations in a thoughtful manner. NPWH will provide leadership to ensure that:
- federal legislators have evidence-based information regarding policies needed to improve contraception access that reduces disparities in individuals’ and couples’ abilities to prevent unintended pregnancies.
- policies support public and private insurance coverage that encompasses prescription, pharmacist-provided, and OTC contraceptives.
- policies do not impose age restrictions on access to prescription, pharmacist-provided, or OTC contraceptives.
- NPs have the resources needed to advocate for access to safe, effective, acceptable, and affordable contraceptives at state and federal levels.
- continuing education programs and resources are available for NPs to lead and contribute meaningfully to developing and evaluating state-level protocols for pharmacy access to HCs.
- research on outcomes related to OTC and pharmacist-provided HCs is encouraged and supported.
References
1. Guttmacher Institute. Fact Sheet: Unintended Pregnancy in the United States. September 2016. guttmacher.org/ sites/default/fi les/factsheet/fb-unintended-pregnancy-us.pdf
2. Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008-2011. New Engl J Med. 2016;374(9):843-852.
3. Mosher WJ, Jones J, Abma J. Nonuse of contraception among women at risk of unintended pregnancy in the United States. Contraception. 2015;92(2):170-176.
4. Grindlay K, Grossman D. Prescription birth control access among U.S. women at risk of unintended pregnancy. J Womens Health. 2016;25(3):249-254.
5. Clare C, Squire MB, Alvarez K, et al. Barriers to adolescent contraception use and adherence. Int J Adolesc Med Health. 2018;30(4):1-8.
6. Chernick LS, Schnall R, Higgins T, et al. Barriers to and enablers of contraceptive use among adolescent females and their interest in an emergency department based intervention. Contraception. 2015;91(3):217-225.
7. Williams RL, Meredith AH, Ott MA. Expanding adolescent access to hormonal contraception: an update on over-the-counter, pharmacist prescribing, and web-based telehealth approaches. Curr Opin Obstet Gynecol. 2018;30(6):458-464.
8. FAQs About Rx-to-OTC Switch. Consumer Healthcare Products Association. 2019. chpa.org/faqsswitchpp.aspx
9. Kaiser Family Foundation. Fact Sheet: Oral Contraceptive Pills. August 2017. files.kff.org/attachment/factsheet-oral-contraceptive-pills.
10. Barot S. Moving oral contraceptives to over-the-counter status: policy versus politics. Guttmacher Pol Rev 2015;18(4):85-91.
11. Hill JD, Hill JM, Gentile NJ. A review of state pharmacist collaborative practice laws. Am J Health Syst Pharm. 2016;73(18):1467-1472.
12. Ibis Reproductive Health. Free the Pill: What’s the Law in Your State? Updated August 2018. freethepill.org/statepolicies/
13. Kaiser Family Foundation. State Requirements for Insurance Coverage of Contraceptives. July 2018. kff.org/ other/state-indicator/state-requirements-for-insurance-coverage-of-contraceptives/?currentTimeframe= 0&sortModel=%7B%22colId%22:%22Location%22,%22 sort%22:%22asc%22%7D
14. Oregon Pharmacists Prescribing of Contraceptive Therapy. oregon.gov/pharmacy/Pages/ContraceptivePrescribing.aspx#Tool-Kit_Resources.
15. Shulman LP. The state of hormonal contraception today: benefi ts and risks of hormonal contraceptives: combined estrogen and progestin contraceptives. Am J Obstet Gynecol. 2011;205(4):S9-S13.
16. Curtis KM, Tepper NK, Jatlaoui TC, et al. U.S. Medical Eligibility Criteria for Contraceptive Use, 2016. MMWR Recomm Rep. 2016;65(3):1-103.
17. Grossman D, Fernandez L, Hopkins K, et al. Accuracy of self-screening for contraindications to combined oral contraceptive use. Obstet Gynecol. 2008;112(3):572-578.
18. Shotorbani S, Miller L, Blough DK, Gardner J. Agreement between women’s and providers’ assessment of hormonal contraception risk factors. Contraception. 2006;73(5):501-506.
19. Doshi JS, French RS, Evans HE, Wilkinson CL. Feasibility of a self-completed history questionnaire in women requesting repeat hormonal contraception. J Fam Plann Reprod Health Care. 2008;34(1):51-54.
20. Gardner JS, Miller L, Downing DF, et al. Pharmacist prescribing of hormonal contraceptives: results of the Direct Access study. J Am Pharm Assoc. 2008;48(2):212-221.
21. American Pharmacists Association. More states address pharmacists’ provider status recognition. April 1, 2015. pharmacist.com/more-states-address-pharmacists-provider-status-recognition
22. Landau SC, Tapias MP, McGhee BT. Birth control within reach: a national survey on women’s attitudes toward an interest in pharmacy access to hormonal contraception. Contraception. 2006;74(6):463-470.
23. Grossman D, Grindlay K, Li R, et al. Interest in over-the-counter access to oral contraceptives among women in the U.S. Contraception. 2013;88(4):544-552.
24. Grindlay K, Grossman D. Interest in over-the-counter access to a progestin-only pill among women in the United States. Womens Health Issues. 2018;28(2):144151.
25. Manski R, Kottke M. A survey of teenagers’ attitudes toward moving oral contraceptives over the counter. Perspect Sex Reprod Health, 2015;47(3):123-129.
26. OCs OTC Working Group. Statement of Purpose. 2019. ocsotc.org/statement-of-purpose/
Approved by the NPWH Board of Directors: March 25, 2019