
Stroke is a debilitating event with lifelong implications for patients and their families. The sooner that symptoms of a stroke are recognized and treatment is initiated, the greater the likelihood that long-term sequelae can be mitigated or even prevented. Even better is preventing stroke before it happens in persons who are at risk.
A stroke is a syndrome of neurologic deficit arising from a vascular disorder that causes brain injury.1 In an ischemic stroke, which accounts for 87% of all strokes, arterial blood flow to the brain is interrupted as a result of a cerebral thrombosis or embolism.1 A transient ischemic attack (TIA) is caused by temporary clots that may presage a full-blown stroke in the future if preventive measures are not instituted. With a TIA, symptoms occur over a short period of time and resolve on their own. A hemorrhagic stroke, which accounts for 13% of all strokes, occurs when a weakened blood vessel ruptures in the setting of hypertension (HTN), an aneurysm, or an arteriovenous malformation.1
Incidence
In the United States, 6.8 million persons are stroke survivors; among these stroke survivors, 3.8 million are women.2 Stroke is the fifth-leading cause of death for men, but the third-leading cause for women.2 In the U.S., more than half (53.5%) of the estimated 795,000 new or recurrent strokes occur in women each year, resulting in about 55,000 more strokes in women than in men. Also, women who have a stroke, compared with their male counterparts, are institutionalized more often and have a poorer recovery and a worse quality of life.2
Symptoms
The National Stroke Association describes stroke symptoms as:
• Sudden numbness or weakness of the face, arm, or leg, usually on one side;
• Sudden confusion, difficulty with speech, or difficulty understanding speech;
• Sudden difficulty seeing with one or both eyes;
• Sudden difficulty walking, dizziness, or loss of balance or coordination; and/or
• Sudden severe headache with no known cause.3
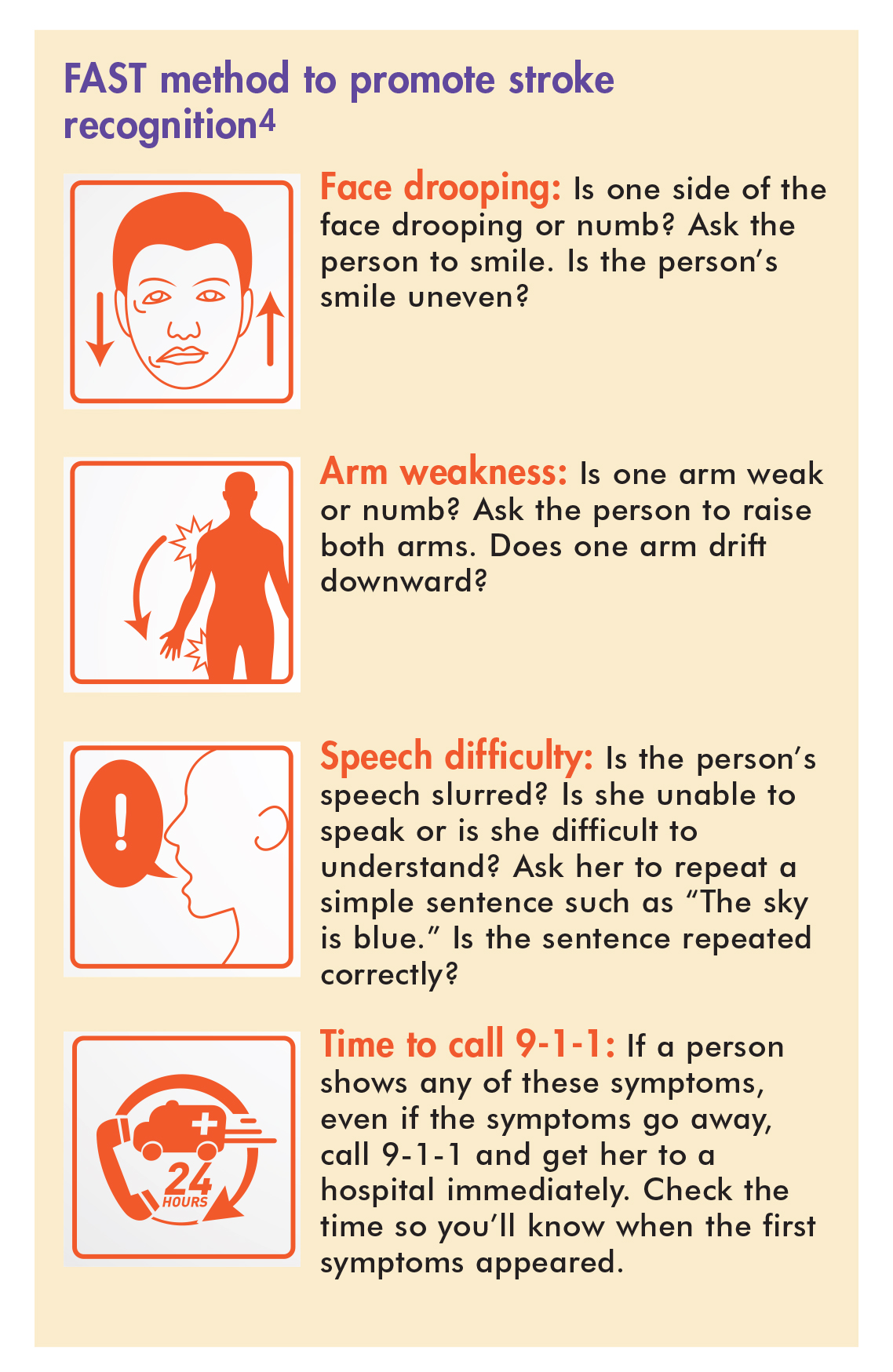
Warning symptoms of a stroke should be known by both healthcare providers (HCPs) and the general public. One measure to promote stroke awareness is the FAST method (Sidebar).4 The key is to quickly recognize a stroke and call 9-1-1 for assistance as needed.
{kind=link}
Risk factors
Many risk factors for stroke, including higher age, physical inactivity, prior cardiovascular disease, obesity, poor diet, smoking, and metabolic syndrome, have a similar prevalence in women and men.2 Other stroke risk factors, including HTN, diabetes mellitus (DM), atrial fibrillation (AF), migraine with aura, depression, and psychosocial stress, are more prevalent and/or more dangerous in women than in men.2 Stroke risk factors that are specific to women include pregnancy, pre-eclampsia, gestational diabetes, combined oral contraceptive (COC) use, and possibly postmenopausal hormone therapy (HT) use.2
Strategies for stroke prevention
These general measures can be taken, as needed, to reduce modifiable stroke risk factors2,5,6:
• Smoking cessation: Smoking cessation is one of the best measures for stroke prevention.
• Lifestyle changes: Following a healthful diet (e.g., Mediterranean diet or DASH diet) and increasing physical activity (at least 40 minutes 3-4 days/week) can help reduce body weight and levels of low-density lipoprotein cholesterol.
• Statin pharmacotherapy: This regimen is recommended for patients with a high 10-year risk for a cardiovascular or cerebrovascular event. HCPs can access a risk calculator here.
• Blood pressure reduction: HTN, more prevalent in women than in men after age 55, is considered the most modifiable risk factor for stroke. Maintaining a normal blood pressure (BP), and undergoing regular screening and treatment of HTN—with lifestyle changes and medication, as needed—are crucial to primary stroke prevention.
• Blood glucose control: DM is a risk factor for stroke.
• Atrial fibrillation control: Depending on a woman’s AF type and risk for hemorrhagic complications, she should be on anticoagulant therapy and possibly low-dose aspirin therapy.
• Avoidance of exogenous estrogen use: This recommendation depends on a woman’s risk/benefit profile.
At-risk pregnant women
To prevent pre-eclampsia, women with chronic primary or secondary HTN or previous pregnancy-related HTN should take low-dose aspirin from the 12th week of gestation until delivery.1 Oral calcium supplementation (≥1 g/day) should be considered for women with low dietary intake of calcium (<600 mg/day). Women with severe HTN in pregnancy should be treated with safe and effective antihypertensives such as methyldopa, labetalol, or nifedipine. Consideration should be given to treating women with moderate HTN in pregnancy—again, with safe and effective antihypertensives. Atenolol, angiotensin receptor blockers, and direct renin inhibitors are contraindicated during pregnancy.
Combined oral contraceptive users
Aggressive therapy of additional stroke risk factors may be reasonable in COC users. Although routine screening for pro-thrombotic mutations before initiation of hormonal contraception is not useful, BP measurement is recommended. COC use may be harmful in women with stroke risk factors such as cigarette smoking or a history of thromboembolic events and should be reconsidered.
Hormone therapy users
Hormone therapy (e.g., conjugated equine estrogens, alone or with medroxyprogesterone) should not be used for primary or secondary prevention of stroke in postmenopausal women. Selective estrogen receptor modulators such as raloxifene and tamoxifen should not be used for primary prevention of stroke.
Migraineurs with aura
Because of the link between higher migraine frequency and stroke risk, treatments to reduce migraine frequency may be reasonable, although evidence is lacking that this approach reduces the risk of a first stroke. Because of the increased stroke risk seen in female migraineurs with aura who smoke, smoking cessation in this group is strongly advised.
Women with atrial fibrillation
Considering the increased prevalence of AF with age and the higher risk of stroke in elderly women with AF, active screening (in particular of women older than 75 years) in primary care settings using pulse taking followed by an ECG is recommended. Oral anticoagulation is not recommended in women aged 65 years or younger with AF alone and no other risk factors. Antiplatelet therapy is a reasonable therapeutic option for selected low-risk women. New oral anticoagulants are a useful alternative to warfarin for prevention of stroke and systemic thromboembolism in women with paroxysmal or permanent AF and pre-specified risk factors who do not have a prosthetic heart valve or hemodynamically significant valve disease, severe renal failure, lower weight, or advanced liver disease.
Women with depression or psychosocial stress
No specific recommendations regarding stroke prevention were provided for this group. More research is needed to establish which women are at greater risk for stroke and which interventions, if any, may be helpful in reducing stroke risk.
Conclusion
Both women and their HCPs need to be able to recognize stroke symptoms and take action as quickly as possible if an ongoing stroke is suspected. For women at risk for stroke, implementing measures that will reduce stroke risk is vital. HCPs caring for women should be particularly alert to the risks that are more prevalent and dangerous in women and those that are specific to women, and should guide these women accordingly in terms of recommending appropriate prophylactic measures.
Janis R. Guilbeau and Cynthia Watson are nursing faculty at the University of Louisiana at Lafayette. The authors state that they do not have a financial interest in or other relationship with any commercial product named in this article.
References
1. Grossman S. Porth C. Porth’s Pathophysiology: Concepts of Altered Health States. 9th ed. Philadelphia, PA: Wolters Kluwer Lippincott Williams & Wilkins; 2014.
2. Bushnell C, McCullough LD, Awad IA, et al., on behalf of the American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Council for High Blood Pressure Research. Guidelines for the Prevention of Stroke in Women: A Statement for Healthcare Professionals From the American Heart Association/ American Stroke Association. Stroke. 2014;45(5):1545-1588.
3. National Stroke Association. Reducing Risk and Recognizing Symptoms. August 2009.
4. National Stroke Association. Act FAST. 2016.
5. CDC. Preventing Stroke: Healthy Living. Page last updated April 30, 2015.
6. Meschia JF, Bushnell C, Boden-Albala B, et al; American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, Council on Functional Genomics and Translational Biology, and Council on Hypertension. Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(12):3754-3832.