
Women’s health nurse practitioners (WHNPs) are a key element in quality, accessible care of women. However, the diversity of these advanced practice registered nurses does not reflect the growing diversity of the United States population. Structural recruitment and retention strategies to address this disparity include policy implementation, student debt prevention, and equitable faculty salaries. With intentional efforts to increase WHNP student and faculty diversity, these specialized nurses can help to decrease healthcare inequity.
Currently, racially diverse groups account for 23.7% of the population in the United States.1 By 2045, people of color (POC) are expected to comprise 50% of this population.2 The increasing racial and ethnic diversification of the US has been met with high rates of healthcare disparities among POC, in general, and among women of color, specifically.3–5 Nurse practitioners are essential members of the healthcare team as they help to reduce healthcare disparities and improve women’s health outcomes.6–8 Yet, despite literature supporting the need for diverse healthcare professionals, women’s health nurse practitioners (WHNPs) and the faculty that prepare them for this role do not reflect this growing patient diversity.5,6 This lack of diversity, inclusion of experiential perspective, and equity in decision making results in lost opportunities of growth within the profession. The purpose of this article is to discuss the need for increased racial and ethnic diversity among WHNPs and to present strategies to achieve equitable representation of historically underrepresented students and faculty to address this need.
History of diversity in institutions of higher education
Diversity efforts aimed at increasing access to historically excluded groups in institutions of higher education (IHEs) have typically been motivated by external mandates. For instance, historically black colleges and universities were established to educate descendants of enslaved people.9 The Morrill Land-Grant College Act of 1862 provided US senators with land to build IHEs for their working class constituents.10 The GI Bill of 1944 broadened educational access for veterans, although qualified Black veterans did not equally benefit from this legislation due, in part, to educational segregation.11 The Supreme Court decision of Brown vs Board of Education in 1954 led to the desegregation of all schools, whereas the Civil Rights Act of 1964 banned admission discrimination based on race, sex, color, religion, or national origin. The Affirmative Action Executive Order of 1961 was amended in 1972 to include the admission of women into IHEs, as the original order focused on government contractors and did not include sex or gender as a category.12
Even with these and other legislations, resistance to the admission of minoritized students persisted at predominantly White institutions until the 1970s and was only mitigated when the federal government and philanthropic foundations threatened to cut their financial support.9 These legislative mandates and policies have compelled student diversity, although gaps persist at the institutional level that sustain existing barriers. Despite federal legislative mandates to help increase the representation among students of color, similar policies legislating recruitment and retainment of faculty of color do not exist.
Racial and ethnic diversity in nursing
Nationally, students of color comprise 51.2% of college students and 35.4% of prelicensure nursing students.13–16 Of interest, those of Hispanic ethnicity account for 27.8% of all college students, making this the largest minoritized group on US college campuses. However, only 12.9% of prelicensure nursing students are Hispanic (Table 1).
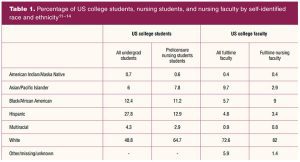
Professors of color comprise less than one-quarter (21.5%) of fulltime faculty.14,15 Compared to all US college faculty, there is a greater racial/ethnic disparity among nursing faculty. For instance, the proportion of Asian/Pacific Islander college faculty is triple that of Asian/Pacific Islander nursing faculty (9.7% vs 2.9%). The only groups in which the racial disparity is greater among all US faculty than among nursing faculty are Black and White faculty. There is a greater percentage of Black nursing faculty (9%) than all Black faculty (5.7%), and a greater percentage of White nursing faculty (82%) than all White faculty (72.6%).
Despite the relative racially diverse makeup of nursing faculty, there is a lag when compared to the demographic composition of students.13,16 The percentage of full-time White nursing faculty is nearly one-third higher than that of White nursing students (82% vs 64.7%), whereas the percentage of nursing faculty of color represent half that of nursing students of color (16.6% vs 35.3%). With a percentage of nursing students nearly four times higher than that of nursing faculty, those who identify as having Hispanic ethnicity have the most disproportionate rate of minoritized nursing students to faculty (12.9% vs 3.4%).13,16
The low percentage of diverse nursing students and faculty may increase their experience of microaggressions—often defined as subtle slights directed toward people from marginalized groups. These experiences, whether within or outside of the classroom, can lead to increased stress and anxiety.17 Service assignments of nursing faculty of color may also be increased compared to that of their White counterparts, a phenomenon often referred to as the “minority tax.”18–20 These and other factors may contribute to the disproportionate promotion rate of minoritized faculty from assistant to associate professors (13%), compared to the promotion rate of White nursing faculty (24%).13
Racial and ethnic underrepresentation among women’s health nurse practitioners
Nationally, there are more than 325,000 nurse practitioners (NPs) with the majority (88.9%) certified in an area of primary care.21 Of this number, only 2.9% have a primary certification in women’s health, compared to 69.7% certified as family nurse practitioners. White NPs are the largest racial group of NPs (86.2%). Those representing POC include Black/African American (9.1%), Hispanic (6.3%), and Asian/Pacific Islander NPs (3.2%) (Table 2).22
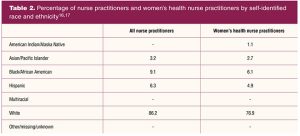
A 2018 survey by the National Association of Nurse Practitioners in Women’s Health assessed the national demographics of WHNPs. More than three-quarters (76.9%) of the total 2,374 respondents self-identified as White. Respondents identifying as POC included 6.1% Black/African American, 4.9% Hispanic, 2.4% Asian, 1.1% American Indian/Alaska Native, and only 0.3% Native Hawaiian/Other Pacific Islander (Table 2).23
When compared, NPs overall have a somewhat higher representation of nurses of color than WHNPs (approximately 18.6% vs 14.8% respectively).16,17 The inequity among minoritized groups is clear. Of interest, registered nurses have a higher POC representation than NPs to include 13.4% Black/African American, 8.7% Asian, and 6.3% Hispanic, comprising a total of 28.4%.16 Thus nurses of color are being lost in the pipeline from RN to NP in general and from RN to WHNP in particular.
How the academic climate impedes diversity among women’s health nurse practitioners
Historically marginalized racial/ethnic groups contend with different forms of microaggressions, a term coined in the 1970s to describe “exclusionary treatments that often did not amount to blatant discrimination, but sometimes escalate to bullying.”24 These can include asking students to speak on behalf of their group during class discussions, undervaluing research performed by faculty of color in communities of color, teaching curricula that centers whiteness and does not integrate diverse perspectives, etc. While these microaggressions in isolation might seem inconsequential, they make for a toxic environment for minoritized faculty and students when compounded. Additionally, organizational climate adversely impacts the recruitment and retention of faculty of color in nursing.25 External mandates and institutional policies tend to leave a gap in addressing harmful behaviors that are often normalized to reinforce hierarchical and power structures.24 Similarly, differences in institutional and individual research funding levels can reinforce systems of scientific oppression and stratification.
Structural recruitment and retention strategies
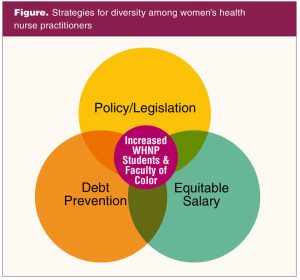
The lack of diversity among WHNPs is a structural issue, thereby requiring both systemic and systematic solutions. Strategies to increase WHNPs of color require intentional interventions throughout the nursing pipeline. In addition to recruitment, retention, mentoring, and academic support of minoritized students and faculty, three categories of structural improvement should also be included.25–32 These areas are policy and regulatory changes, debt prevention, and equitable salaries (Figure).
Policy change implementation
Regional and discipline-specific accreditation agencies are increasingly more explicit about diversity as evaluation criteria, although it remains to be seen whether these efforts go far enough to make significant change in the phenotypic landscape of IHE.33 Nursing school accreditation bodies, including the Accreditation Commission for Education in Nursing, the Commission on the Collegiate Nursing Education, and the Commission for Nursing Education Accreditation, should ensure schools of nursing have objective measures to assess institutional policies, processes, and approaches toward addressing systemic racism.34 Measures should include a comprehensive evaluation of nursing school curricula, climate, and efforts to increase student and faculty diversity to better reflect the communities in which they learn and teach.34
This would maintain congruence with the Future of Nursing 2020–2030’s recommendation to “ensure that nurses are prepared to address social determinants of health and achieve health equity,” and build on the ongoing commitment to diversify the nursing workforce.
Student debt prevention
Entry to WHNP practice may occur by earning a Master of Science in Nursing degree, post-master’s certificate, or Doctor of Nursing Practice degree. In 2021, the average US public four-year and private nonprofit four-year graduate tuition costs were $8,680 and $29,960 for master’s level students and $10,830 and $42,920 for doctoral students, respectively.35 During the 2019–2020 academic year, the average respective cost of tuition at four-year public and private universities was $25,094 and $47,010.36 These public and private costs represent an increase of $2,702 and $5,403 over the previous academic year.
Where scholarships and grants are not enough to cover growing tuition costs, students rely on academic loans to cover the remaining cost. Excluding Asian students, racially minoritized college graduates have more educational debt than their White counterparts.14,37 Black students have the highest debt among students of color at time of graduation.14 Thus, educational scholarships and grants may aid in the recruitment of diverse students, particularly among Black candidates.
Many professional nursing organizations provide scholarships for nurses seeking NP education. Hospitals and other healthcare facilities may also provide tuition reimbursement for nurses who enroll in graduate programs. However, the desire to provide equal access to education funding must expand to the provision of equitable access for this funding. Equity is attained by helping to close the funding and wealth gaps between nurses of color and their counterparts. This can be achieved through the creation and ongoing funding of local and national scholarships and loan forgiveness program created specifically for WHNP students of color, such as those provided by Vanderbilt University, the National Black Nurses Association, and the Health Resources and Services Administration.38–40
Equitable faculty salaries
One barrier in attracting advanced practice registered nurses (APRNs) into academic positions is the academic-practice salary gap. The mean salary of a registered nurse with a bachelor’s degree ($77,460) is comparable to that of nursing faculty ($83,160). However, this price point is much lower than the mean salary of certified nurse midwives, certified registered nurse anesthetists, and certified nurse practitioners ($115,800).41 APRNs who desire to work in academia must contend with a $30,000 or more reduction in salary, which may be a significant barrier to this career change, especially for APRNs of color.
In 37% of nursing schools surveyed, significant salary difference was identified as the main difficulty in recruiting new faculty.13 This change in salary may be felt more by people of color, especially Black people, who have a lower rate of marriage and a higher rate of solo, non-cohabiting parenting.42,43 All faculty positions, not only those held by faculty of color, should be financially incentivized to attract and retain faculty, and not prevent them from moving into academia. Furthermore, salary equity among similarly ranked faculty is necessary to prevent minoritized faculty from being paid at the lowest end of the salary scale.44 Finally, pay equity among newly hired and established faculty should be established and the process for salary offers and merit increases should be transparent.
Final thoughts
The paucity of certified WHNPs of color underscores the need of policies and legislation supporting WHNP practice, a full understanding of the depth and breadth of the WHNP’s contribution to healthcare, and an increase of WHNP education programs. These strategies should not proceed without attention given to the increased number of nursing students and faculty of color. Although accreditation agencies may become more explicit about diversity, WHNP programs need to continually review their recruitment and educational practices for diversity, equity, and inclusion.33 Financial support, by means of scholarships for students and faculty salaries that are on par with nurse clinicians, should be provided to increase equity among WHNP students and faculty of color.
Conclusion
The social contract of the nursing academy is to educate the next generation of professionals to solve pressing health problems and advance healthcare. WHNPs have a history of providing healthcare to underserved and marginalized populations, and the goal of providing care to the most vulnerable should be maintained. To effectively accomplish this goal in the next millennia, diversity among WHNPs must reflect the diversity of the communities they serve.
This article has presented several practical methods that, when implemented, may increase diversity among US WHNP students and faculty. Diversity, however, does not begin or end with racial/ethnic differences. Future discussions on WHNP diversity should integrate the intersectionality prism to include age and gender diversity among faculty, as well as the inclusion of rural and nontraditional students. To properly understand and serve diverse populations, WHNPs should reflect that same diversity. With increased intention, diversity among WHNPs can be achieved.
Tiffany M. Montgomery is Assistant Professor at Temple University College of Public Health in Philadelphia, Pennsylvania. Patience N. Ajoff-Foster is Executive Director in the Drexel University Office of Equality and Diversity in Philadelphia. Shawana S. Moore is Assistant Professor at the Thomas Jefferson University College of Nursing in Philadelphia, and Nalo M. Hamilton is Associate Professor at the University of California, Los Angeles School of Nursing in Los Angeles, California. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
References
- U.S. Census Bureau. QuickFacts: United States. 2019.
- U.S. Census Bureau. Older people projected to outnumber children for the first time in U.S. history. 2018.
- Reed D. Racial disparities in healthcare: how COVID-19 ravaged one of the wealthiest African American counties in the United States. Soc Work Public Health.2021;36(2):118-127.
- Petersen EE, Davis NL, Goodman D, et al. Racial/ethnic disparities in pregnancy-related deaths—United States, 2007–2016. Morb Mortal Wkly Rep. 2019;68(35):762.
- Artiga S, Orgera K, Pham O. Disparities in Health and Health Care: Five Key Questions and Answers. Henry J. Kaiser Family Foundation; 2020:13.
- Poghosyan L, Carthon JMB. The untapped potential of the nurse practitioner workforce in reducing health disparities. Policy Polit Nurs Pract.2017;18(2):84-94.
- American Association of Nurse Practitioners. Quality of Nurse Practitioner Practice. American Association of Nurse Practitioners. Revised 2020.
- Pair LS, Hodges AL, Holland AC. How nurse practitioners can affect women’s health in rural America. Women’s Healthcare. 2020;8(1):47-49.
- Kean M. Desegregating Private Higher Education in the South: Duke, Emory, Rice, Tulane, and Vanderbilt. LSU Press; 2008.
- Rogers WW. The founding of Alabama’s land grant college at Auburn. Ala Rev. 2016;69(1):54-77.
- McCardle T. A promise deferred: Black veterans’ access to higher education through the GI Bill at the University of Florida, 1944–1962. Educ Stud. 2017;53(2):122-134.
- Wilder J, Osborne-Lampkin L, Jackson EN. Rearticulating Black faculty diversity efforts in the age of “postracialism” and Obama. West J Black Stud. 2015;39(3).
- National League for Nursing. Nursing education statistics. 2021.
- National Center for Education Statistics. Digest of Education Statistics, 2019. National Center for Education Statistics; 2020.
- Taylor M, Turk JM, Chessman HM, Espinosa LL. Race and Ethnicity in Higher Education: 2020 Supplement. American Council on Education; 2020.
- American Association of Colleges of Nursing. Race/ethnicity of students enrolled from generic (entry-level) baccalaureate, RN-to-baccalaureate, total baccalaureate, master’s, research-focused doctoral, and DNP programs in nursing, 2010-2019 (Table). 2020.
- Ro K, Villarreal J. Microaggression in academia: consequences and considerations. Nurs Educ Perspect. 2021;42(2):120-121.
- Guillaume RO, Apodaca EC. Early career faculty of color and promotion and tenure: the intersection of advancement in the academy and cultural taxation. Race Ethn Educ. 2020;0(0):1-18.
- Trejo J. The burden of service for faculty of color to achieve diversity and inclusion: the minority tax. Mol Biol Cell. 2020;31(25):2752-2754.
- Williamson T, Goodwin CR, Ubel PA. Minority tax reform—avoiding overtaxing minorities when we need them most. N Engl J Med. 2021;384(20):1877-1879.
- American Association of Nurse Practitioners. NP Fact Sheet. Updated May 2021.
- U.S. Bureau of Labor Statistics. Employed persons by detailed occupation, sex, race, and Hispanic or Latino ethnicity. 2020.
- National Association of Nurse Practitioners in Women’s Health. 2018 NPWH women’s health nurse practitioner workforce demographics and compensation survey: Highlights report.
- Anderson MR, Young KS. Fix Your Climate: A Practical Guide to Reducing Microaggressions, Microbullying, and Bullying in the Academic Workplace.2020.
- Hamilton N, Haozous EA. Retention of faculty of color in academic nursing. Nurs Outlook. 2017;65(2):212-221.
- Iheduru-Anderson K. Barriers to career advancement in the nursing profession: perceptions of Black nurses in the United States. Nurs Forum (Auckl). 2020;55(4):664-677.
- Brewer B. The lack of diversity in advanced nursing. Nurse Practitioner Schools. September 4, 2020.
- Murray TA, Pole DC, Ciarlo EM, Holmes S. A nursing workforce diversity project: Strategies for recruitment, retention, graduation, and NCLEX-RN success. Nurs Educ Perspect. 2016;37(3):138-143.
- Tranter S, Gaul C, McKenzie S, Graham K. Initiatives aimed at retaining ethnically diverse student nurses in undergraduate programmes: An integrative review. J Clin Nurs. 2018;27(21-22):3846-3857.
- Woods-Giscombe CL, Johnson Rowsey P, Kneipp S, et al. Student perspectives on recruiting underrepresented ethnic minority students to nursing: enhancing outreach, engaging family, and correcting misconceptions. J Prof Nurs. 2020;36(2):43-49.
- Gates SA. What works in promoting and maintaining diversity in nursing programs. Nurs Forum (Auckl). 2018;53(2):190-196.
- Breslin ET, Nuri-Robins K, Ash J, Kirschling JM. The changing face of academic nursing: nurturing diversity, inclusivity, and equity. J Prof Nurs. 2018;34(2):103-109.
- Healey L. Do U.S. accrediting agencies do enough to assess diversity efforts? Insight into Diversity. October 26, 2016.
- National Academies of Health. The Future of Nursing 2020-2030 | National Academies. 2021.
- Song J. Average cost of college in America. ValuePenguin. January 11, 2021.
- Sallie Mae. How America Pays for College. 2020.
- U.S. Census Bureau. American Community Survey. 2020.
- Vanderbilt University. Minority Students Financial Information. 2021.
- National Black Nurses Association. Scholarship Program. 2021.
- Bureau of Health Workforce. Apply to the Faculty Loan Repayment Program. May 2021.
- U.S. Bureau of Labor Statistics. Occupational Outlook Handbook. 2020.
- Mayol-García Y, Gurrentz B, Kreider RM. Number, Timing, and Duration of Marriages and Divorces: 2016:34.
- Pew Research Center. Facts On Unmarried Parents in the U.S. Pew Research Center’s Social & Demographic Trends Project. April 25, 2018.
- Flaherty C. New data on faculty representation, pay. High Ed. Published online March 25, 2020.
KEY WORDS: diversity, nursing education, advanced practice, women’s health nurse practitioner, recruitment, retention
Womens Healthcare. 2022;10(2):19-25. doi:10.51256/WHC042219