
Because multiple subjective factors can cloud the diagnosis of polycystic ovary syndrome, anti-Müllerian hormone (AMH) level, an objective value, has been studied as a potential supplement to polycystic ovarian morphology in diagnosing and managing the syndrome. The author reviews recent evidence demonstrating the role of AMH in this regard.
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder affecting females of reproductive age and the leading cause of anovulatory infertility.1 Lack of correct diagnosis and management of PCOS can lead to reproductive challenges (e.g., infertility, early miscarriage, gestational diabetes), metabolic disorders (e.g., type 2 diabetes mellitus), or cardiovascular disorders (e.g., hypertension, dyslipidemia).2 Advanced practice nurses (APNs) are tasked with correctly diagnosing and managing PCOS in order to prevent these associated morbidities, which can compromise quality of life.
According to the Rotterdam criteria for diagnosing PCOS, at least two of these three elements must be met: clinical and/or biochemical hyperandrogenism, ovulatory dysfunction, and polycystic ovarian (PCO) morphology.3 PCO morphology has been defined as the presence of more than 12 follicles measuring <10 mm and/or an increased ovarian volume (>10 mL) without a cyst or dominant follicle in either ovary.3 According to Lujan et al,4 the inclusion of ultrasonographic(USG) evidence of polycystic ovaries as a diagnostic marker has substantially broadened the phenotypic spectrum of PCOS, yet much debate surrounds the validity of these newly identified milder variants of the syndrome.
In light of such concerns, the use of anti-Müllerian hormone (AMH) level as a more reliable marker for PCO morphology than follicle size and number on USG has been investigated in recent studies. Results of these studies indicate a consistent relationship between AMH level and USG estimates of antral follicle count (AFC) and ovarian volume.5-7 Research has shown that serum AMH levels are significantly increased in women with PCOS versus those without PCOS.1,5,6 Although further research is needed, serum AMH measurement may prove to be a useful tool for APNs in diagnosing phenotypes of PCOS that satisfy the Rotterdam criteria.
Development of polycystic ovaries
To appreciate the role of AMH in PCOS, APNs must understand the two-cell, two-gonadotropin model of estrogen synthesis, as well as how disruption of this process may lead to development of polycystic ovaries.8 This model describes the working hormonal balance between the outer theca cell layer and the inner granulosa cell layer in the ovarian follicle; the former cell layer secretes androgens and the latter, estrogens. When luteinizing hormone (LH) stimulates cholesterol in the theca cells, androgen is released. Upon exposure to follicle- stimulating hormone (FSH), androgen is converted into estrogens in the granulosa cells.
When this two-cell, two-gonadotropin process is disrupted, a hormonal imbalance ensues, such that circulating LH concentrations exceed FSH concentrations. Ovarian androgen production increases, resulting in serum androgen excess. The increased androgen stimulates the growth of smaller antral follicles yet inhibits later follicular development and maturation.9 Such arrest in follicle growth can lead to PCO morphology. These smaller antral follicles cannot be released via ovulation or subsequent luteinization.
Function of AMH
Anti-Müllerian hormone has been identified as the hormone secreted by sertoli cells in the male testes during embryonic sexual differentiation.10,11 In females, AMH is a glycoprotein produced by the granulosa cells of antral follicles. The highest level of AMH secretion is evident in antral follicles ≥4 mm in diameter and continues to be expressed until the differentiation stage (8-9 mm), in which FSH selects a dominant follicle for future ovulation.12 Evidence suggests that AMH inhibits follicular growth by inhibiting estrogen secretion in the antral follicles prior to FSH selection. As a result, estrogen and AMH have an inverse relationship; AMH exerts a regulatory function by ensuring that not all primordial follicles are released at once.13
Levels of AMH fluctuate only minimally throughout the menstrual cycle, and not to the same extent as FSH and other pituitary and ovarian hormone levels. AMH levels are noted to be lower in women during pregnancy. These levels decline steadily after age 25 and are undetectable after menopause.14 Information on whether AMH levels are affected by the use of hormonal contraception is conflicting.15,16
Current uses of AMH measurement
Because AMH is secreted by antral follicles prior to the differentiation stage, it is most often used as a clinical biomarker for ovarian reserve in infertility diagnosis and management and in detection of premature ovarian aging.17,18 AMH is an excellent predictor of ovarian responsiveness in ovulation induction and in vitro fertilization, as well as a useful tool to help predict ovarian hyper-stimulation, oocyte yield, and ovarian function pathology in an infertility setting.13,19-21 In addition, AMH may be useful in assessing the need for fertility-preservation strategies and detecting post-chemotherapy or surgical damage to the ovarian reserve.13,22
Use of AMH measurement in diagnosing PCOS
A thorough history, physical examination, and select laboratory tests are important elements in determining the presence of androgen excess and ovulatory dysfunction— two of the three Rotterdam criteria used for PCOS diagnosis.3 As described earlier, polycystic ovaries, the third criterion, are identified via USG by the presence of more than 12 antral follicles measuring <10 mm and/or an increased ovarian volume (>10 mL) without a cyst or dominant follicle in either ovary. However, USG has potential shortcomings, including sensitivity of the machine, less-than-perfect operator technique, and subjective interpretation of the findings. In addition, transvaginal USG imaging may be inappropriate or less accurate in certain patient populations (e.g., obese persons or those who have never been sexually active).3,4
Determination of a patient’s AMH level, an objective laboratory value, may help minimize the subjectivity of the USG findings. In several studies, a serum AMH level >18 pmol/L, when compared with USG, provided better sensitivity and specificity for PCO morphology in women who met Rotterdam criteria for PCOS.5,23,24 Other studies have been performed to determine the optimal cutoff for the AMH value:
• A meta-analysis of data extracted up until January 2013 showed that an AMH value of 33.6 pmol/L was 82.8% sensitive and 79.4% specific in diagnosing PCOS in symptomatic women.25
• In 2013, a study of 60 infertile women with PCOS showed that an AMH value of 23.8 pmol/L was 98% sensitive and 93% specific in diagnosing PCOS.26
• Another 2013 study, conducted on 59 infertile women, 37 of whom had characteristics of PCOS, showed that an AMH level of 33 pmol/L was 95% sensitive and 95% specific in diagnosing PCOS.1
• In a study conducted in 2011 on 240 patients, an AMH value of 35.7 pmol/L was 92% sensitive and 97% specific in identifying PCO morphology.5
These findings notwithstanding, a standard AMH level for diagnosing PCOS has yet to be established. Furthermore, several limitations preclude AMH from becoming widely utilized for PCOS diagnosis. First, lack of a universally accepted method and assay to measure AMH prevents it from becoming an established diagnostic tool for PCOS.27 Second, because AMH declines with advancing age, the threshold for PCOS diagnosis may need to be modified through the life span.28 Third, research involving the use of AMH level to diagnose PCOS in adolescents is limited.27, 29, 30 Finally, the 2013 Endocrine Society guidelines do not include a recommendation for using AMH measurement as a routine diagnostic tool for PCOS.3
Although AMH level and oligoanovulation are correlated, AMH has not been proven to be an acceptable indicator of ovulatory dysfunction or hyper androgenism.23 Hence, AMH level, if used, should be combined with other laboratory or clinical measures of hyperandrogenism and/or ovulatory dysfunction to maximize its diagnostic sensitivity and specificity. Furthermore, the role of AMH is unclear in diagnosing subtypes of PCOS, especially those that do not present with classic symptoms. Studies have suggested that ovulatory PCOS phenotypes, compared with anovulatory types, are associated with differing levels of serum AMH.31
Use of AMH measurement in gauging response to PCOS treatment
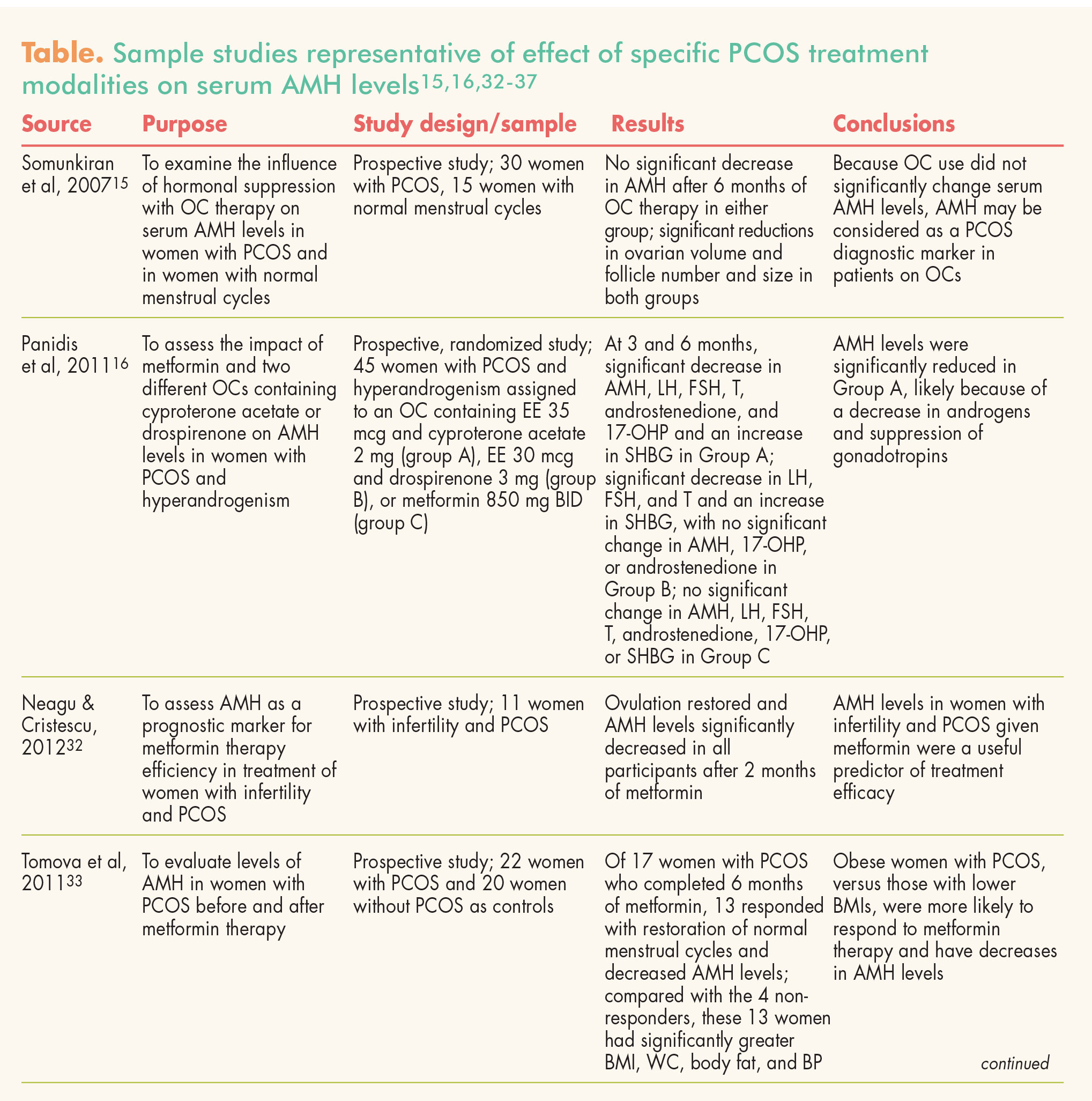
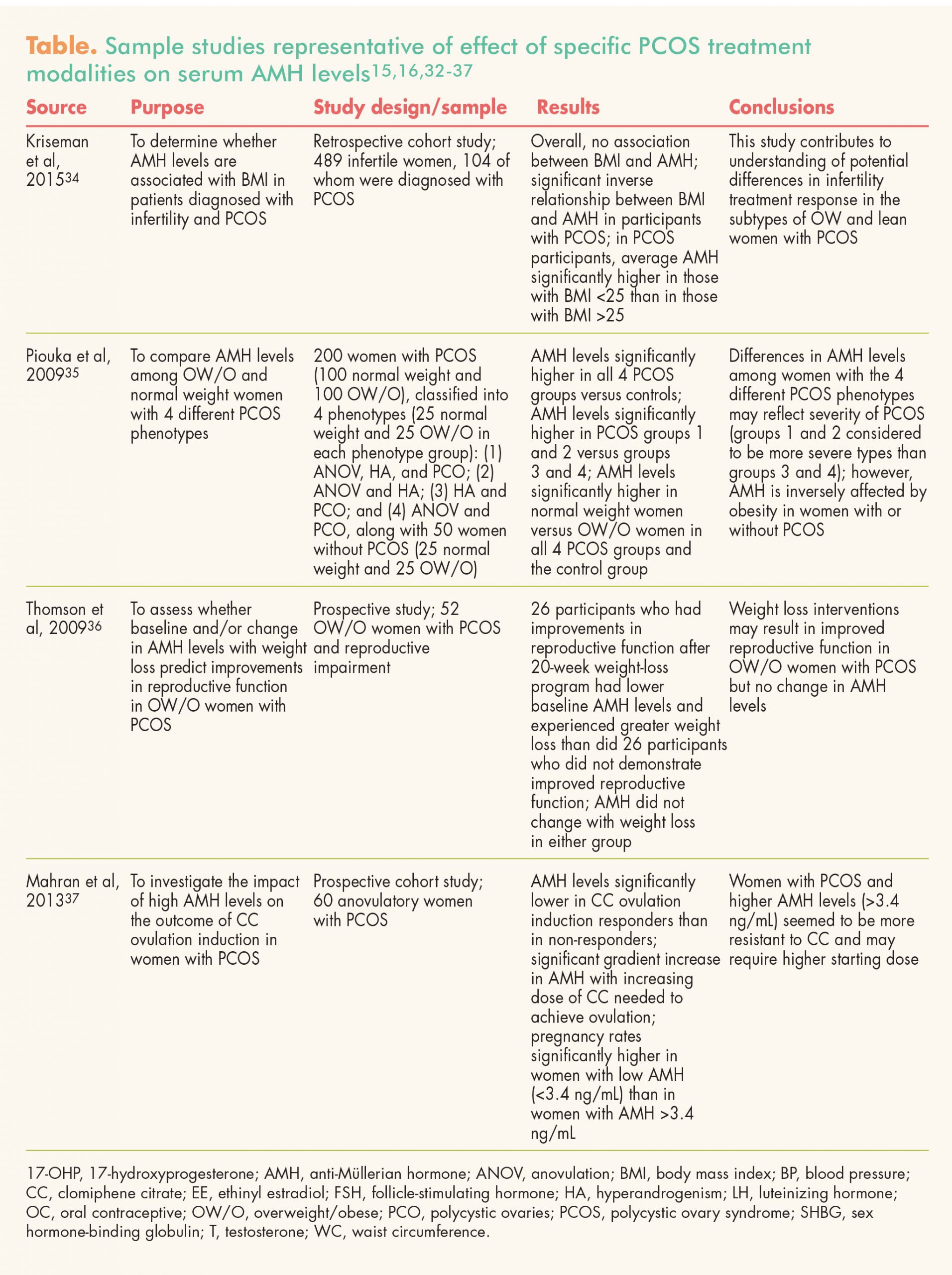
The goal of PCOS treatment is managing symptoms and minimizing co-morbidities. Proper management can reduce the risk for certain gynecologic cancers and infertility. Management should be both individualized and holistic and may include weight reduction through lifestyle modification and use of hormonal contraceptives, metformin, and gonadotropin/estrogen modulators. Current methods of monitoring the effectiveness of these management modalities include patient-reported symptom improvement and menstrual regulation, physical examination for reduction in signs of hyperandrogenism, measurement of insulin and glucose levels, and achievement of successful pregnancy outcome.
Many recent studies have been conducted to assess the relationship between various PCOS management modalities and patients’ AMH levels; the Table (pp 38–39) lists a representative sample of such studies.15, 16, 32-37 Additional research is needed to demonstrate the utility of these AMH measurements, especially as compared with current methods (e.g., clinical signs, patient-reported symptoms, other lab test findings) in making decisions about and evaluating the effectiveness of treatment.
{kind=link}
{kind=link}
Discussion
Based on what is known at this time, use of the AMH level is not recommended as a replacement for any component of the Rotterdam criteria in terms of diagnosing PCOS or as an assessment tool for monitoring the success of existing management modalities. However, AMH may be a useful supplemental tool for APNs because it is an objective and more reliable marker for diagnosing PCO morphology. Indeed, AMH can help providers who are not trained in pelvic or transvaginal USG in diagnosing PCOS. Although more research is needed in this area, AMH may be another component of PCOS diagnosis and management in the future.
Conclusion
Although the Rotterdam criteria are the gold standard for diagnosing PCOS, concern regarding the subjective nature of polycystic morphology on USG has been voiced over the years. An AMH value >35 pmol/L may have the highest sensitivity and specificity in terms of indicating polycystic ovaries. However, data supporting the use of AMH levels to make treatment choices or to monitor the effectiveness of such treatments in females with PCOS are inconclusive. At the very least, findings from studies assessing changes in AMH levels related to specific treatment modalities may offer more insight into the pathophysiology of this complex endocrine disorder.
Tiffany A. Tseng is a women’s health nurse practitioner at HRC Fertility in Pasadena, California. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
1. Casadei L, Madrigale A, Puca F, et al. The role of serum anti-Müllerian hormone (AMH) in the hormonal diagnosis of polycystic ovary syndrome. Gynecol Endocrinol. 2013;29(6):545-550.
2. Jayasena CN, Franks S. The management of patients with polycystic ovary syndrome. Nat Rev Endocrinol. 2014;10(10):624-636.
3. Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98(12):4565-4592.
4. Lujan ME, Chizen DR, Pierson RA. Diagnostic criteria for polycystic ovary syndrome: pitfalls and controversies. J Obstet Gynaecol Can. 2008;30(8):671-679.
5. Dewailly D, Gronier H, Poncelet E, et al. Diagnosis of polycystic ovary syndrome (PCOS): revisiting the threshold values of follicle count on ultrasound and of the serum AMH level for the definition of polycystic ovaries. Hum Reprod. 2011;26(11):3123-3129.
6. Pigny P, Merlen E, Robert Y, et al. Elevated serum level of anti-mullerian hormone in patients with polycystic ovary syndrome: relationship to the ovarian follicle excess and to the follicular arrest. J Clin Endocrinol Metab. 2003;88(12):5957-5962.
7. Piltonen T, Morin-Papunen L, Koivunen R, et al. Serum anti-Müllerian hormone levels remain high until late reproductive age and decrease during metformin therapy in women with polycystic ovary syndrome. Hum Reprod. 2005;20(7):1820-1826.
8. Hillier SG, Whitelaw PF, Smyth CD. Follicular oestrogen synthesis: the ‘two-cell, two-gonadotrophin’ model revisited. Mol Cell Endocrinol. 1994; 100(1-2):51-54.
9. Vendola KA, Zhou J, Adesanya OO, et al. Androgens stimulate early stages of follicular growth in the primate ovary. J Clin Invest. 1998; 101(12):2622-2629.
10. La Marca A, Stabile G, Artenisio AC, Volpe A. Serum anti-Mullerian hormone throughout the human menstrual cycle. Hum Reprod. 2006; 21(12):3103-3107.
11. Vigier B, Picard JY, Tran D, et al. Production of anti-Müllerian hormone: another homology between Sertoli and granulosa cells. Endocrinology. 1984;114(4):1315-1320.
12. Weenen C, Laven JS, Von Bergh AR, et al. Anti-Müllerian hormone expression pattern in the human ovary: potential implications for initial and cyclic follicle recruitment. Mol Hum Reprod. 2004;10(2):77-83.
13. Dewailly D, Andersen CY, Balen A, et al. The physiology and clinical utility of anti-Müllerian hormone in women. Hum Reprod Update. 2014;20(3):370-385.
14. Leader B, Baker V. Maximizing the clinical utility of antimullerian hormone testing in women’s health. Curr Opin Obstet Gynecol. 2014;26(4):226-236.
15. Somunkiran A, Tavuz T, Yucel O, Ozdemir I. Anti-Müllerian hormone levels during hormonal contraception in women with polycystic ovary syndrome. Eur J Obstet Gynecol Reprod Biol. 2007;134(2):196-201.
16. Panidis D, Georgopoulos NA, Piouka A, et al. The impact of oral contraceptives and metformin on anti-Müllerian hormone serum levels in women with polycystic ovary syndrome and biochemical hyperandrogenemia. Gynecol Endocrinol. 2011; 27(8):587-592.
17. van Rooij IA, Broekmans FJ, Scheffer GJ, et al. Serum antimullerian hormone levels best reflect the reproductive decline with age in normal women with proven fertility: a longitudinal study. Fertil Steril. 2005;83(4):979-987.
18. Lie Fong S, Schipper I, Valkenburg O, et al. The role of anti-Müllerian hormone in the classification of anovulatory infertility. Eur J Obstet Gynecol Reprod Biol. 2015;186:75-79.
19. van Rooij IA, Broekmans FJ, te Velde ER, et al. Serum anti-Müllerian hormone levels: a novel measure of ovarian reserve. Hum Reprod. 2002;17(12):3065-3071.
20. Amer SA, Mahran A, Abdelmaged A, et al. The influence of circulating anti-Müllerian hormone on ovarian responsiveness to ovulation induction with gonadotrophins in women with polycystic ovarian syndrome: a pilot study. Reprod Biol Endocrinol. 2013;11:115.
21. Dąbkowska-Huć A, Lemm M, Sikora J, et al. Anti-Müllerian hormone dynamics during ovulation induction treatment with recombinant follicle-stimulating hormone in women with polycystic ovary syndrome. Endokrynol Pol. 2013; 64(3):203-207.
22. Dunlop CE, Anderson RA. Uses of anti-Müllerian hormone (AMH) measurement before and after cancer treatment in women. Maturitas. 2015;80(3):245-250.
23. Sahmay S, Aydin Y, Oncul M, Senturk LM. Diagnosis of polycystic ovary syndrome: AMH in combination with clinical symptoms. J Assist Reprod Genet. 2014;31(2):213-220.
24. Lauritsen MP, Bentzen JG, Pinborg A, et al. The prevalence of polycystic ovary syndrome in a normal population according to the Rotterdam criteria versus revised criteria including anti-Mullerian hormone. Hum Reprod. 2014;29(4):791-801.
25. Iliodromiti S, Kelsey TW, Anderson RA, Nelson SM. Can anti-Mullerian hormone predict the diagnosis of polycystic ovary syndrome? A systematic review and meta-analysis of extracted data. J Clin Endocrinol Metab. 2013;98(8):3332-3340.
26. Saikumar P, Selvi VK, Prabhu K, et al. Anti mullerian hormone: a potential marker for recruited non growing follicle of ovarian pool in women with polycystic ovarian syndrome. J Clin Diagn Res. 2013;7(9):1866-1869.
27. Dewailly D, Lujan ME, Carmina E, et al. Definition and significance of polycystic ovarian morphology: a task force report from the Androgen Excess and Polycystic Ovary Syndrome Society. Hum Reprod Update. 2014;20(3):334-352.
28. Zec I, Tislaric-Medenjak D, Megla ZB, Kucak I. Anti-Müllerian hormone: a unique biochemical marker of gonadal development and fertility in humans. Biochem Med (Zagreb). 2011;21(3):219-230.
29. Cengiz H, Ekin M, Dagdeviren H, et al. Comparison of serum anti-Müllerian hormone levels in normal weight and overweight-obese adolescent patients with polycystic ovary syndrome. Eur J Obstet Gynecol Reprod Biol. 2014;180:46-50.
30. Pinola P, Morin-Papunen LC, Bloigu A, et al. Anti-Müllerian hormone: correlation with testosterone and oligo- or amenorrhoea in female adolescence in a population-based cohort study. Hum Reprod. 2014; 29(10):2317-2325.
31. Alebić MS, Stojanović N, Duhamel A, Dewailly D. The phenotypic diversity in per-follicle anti-Müllerian hormone production in polycystic ovary syndrome. Hum Reprod. 2015;30(8):1927-1933.
32. Neagu M, Cristescu C. Anti-Müllerian hormone—a prognostic marker for metformin therapy efficiency in the treatment of women with infertility and polycystic ovary syndrome. J Med Life. 2012;5(4):462-464.
33. Tomova A, Deepinder F, Robeva R, et al. Anti-Müllerian hormone in women with polycystic ovary syndrome before and after therapy with metformin. Horm Metab Res. 2011;43(10):723-727.
34. Kriseman M, Mills C, Kovanci E, et al. Antimullerian hormone levels are inversely associated with body mass index (BMI) in women with polycystic ovary syndrome. J Assist Reprod Genet. 2015;32(9):1313-1316.
35. Piouka A, Farmakiotis D, Katsikis I, et al. Anti-Mullerian hormone levels reflect severity of PCOS but are negatively influenced by obesity: relationship with increased luteinizing hormone levels. Am J Physiol Endocrinol Metab. 2009;296(2):E238-E243.
36. Thomson RL, Buckley JD, Moran LJ, et al. The effect of weight loss on anti-Müllerian hormone levels in overweight and obese women with polycystic ovary syndrome and reproductive impairment. Hum Reprod. 2009;24(8):1976-1981.
37. Mahran A, Abdelmaged A, El-Adawy AR, et al. The predictive value of circulating anti-Müllerian hormone in women with polycystic ovarian syndrome receiving clomiphene citrate: a prospective observational study. J Clin Endocrinol Metab.