
Current evidence-based guidelines support the use of statin drugs for primary prevention of cardiovascular (CV) events based on individual CV risk profiles rather than on target cholesterol levels. The purpose of this article is to increase awareness of the impact of CV disease in women and to discuss evidence-based guidelines for the use of statin drugs to decrease CV events in this population.
 line has leveled off, especially among women younger than 55 years.1 Women who are at risk for developing cardiovascular disease (CVD)—a large percentage of the female population—are less likely than their male counterparts to receive preventive treatment.2 If at-risk women are prescribed preventive treatment, it is generally less aggressive than that prescribed for men, and less likely to achieve optimal results.2
line has leveled off, especially among women younger than 55 years.1 Women who are at risk for developing cardiovascular disease (CVD)—a large percentage of the female population—are less likely than their male counterparts to receive preventive treatment.2 If at-risk women are prescribed preventive treatment, it is generally less aggressive than that prescribed for men, and less likely to achieve optimal results.2Women have many of the same risk factors for CVD as do men, including non-modifiable risk factors such as age and family history and modifiable ones such as smoking, overweight/obesity, physical inactivity, hypertension, dyslipidemia, and diabetes mellitus (DM).1 Additional risk factors specific to women include history of preterm delivery, hypertensive pregnancy disorders, gestational diabetes, persistence of weight gain after pregnancy, and menopause. Autoimmune diseases, more common in women than in men, as well as radiation and chemotherapy for breast cancer, also increase CVD risk in women. Depression, especially in younger women, increases the lifelong risk of developing CVD.
In an October 2018 opinion, the American College of Obstetricians and Gynecologists (ACOG) stated that women’s healthcare providers (HCPs) have an opportunity to influence the health of women across the lifespan.3 ACOG recommends including preventive health screening and counseling in routine wellness checkups for women of all ages.3 Women’s healthcare visits should include a comprehensive personal and family health history and assessment of personal risk factors, including those for CVD.
Statin overview
One of the major treatable causes of CVD and stroke is dyslipidemia. Recent reports support the efficacy of prescribing statins to treat dyslipidemia and prevent CVD events.4 Based on a hallmark 2013 guideline for managing blood cholesterol levels, the American College of Cardiology (ACC) reported that 56 million adults aged 40-75 years in the United States were eligible for statin therapy.5,6 With the growing and aging population in the U.S., this number is no doubt even higher in 2019.
Over the years, treatment with statins has focused on reaching a person’s target low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) levels, which are based on a personal CVD risk profile (more on this later).5 Recent reports have supported a change in dyslipidemia treatment focus, with an emphasis on primary and secondary prevention of CV events in persons at risk for them and prescribing statins to certain populations.7 In 2017, guidelines for treatment of elevated cholesterol levels from the ACC and the American Heart Association (AHA) suggested a fundamental shift in hyperlipidemia treatment from focusing mainly on LDL-C values to using appropriate statin dosages in target benefit groups.7 Based on this hallmark publication by the ACC/AHA, many more women now qualify for treatment with statins based on risk determinations. In addition, the new guidelines support less use of the older non-statin drugs (e.g., fibrates, nicotinic acid, bile-acid sequestrants).7
Significant reduction of CV morbidity/mortality with statin drug use has been reported in multiple randomized controlled trials. Statins improve dyslipidemia, reduce the risk of myocardial events, lower stroke risk, reduce LDL-C and triglyceride levels, and raise HDL-C levels.8
Highor moderate-dosage statins, with the choice of dosage depending on a person’s 10-year CVD risk, are used for primary CVD prevention (i.e., prevention of CVD and CVD-related events in persons who have never had CVD). Use of statins as secondary CVD prevention (i.e., to reduce the impact of CVD in individuals who already have the disease) is supported by findings of a reduced risk of major CV events with statin treatment and achievement of low levels of LDL-C, non-HDL-C, and apolipoprotein B, an atherogenic lipoprotein.8
Risk assessment
The 2018 Prevention Guidelines Tool CV Risk Calculator, developed by the ACC/AHA, is used to estimate a person’s 10-year atherosclerotic cardiovascular disease (ASCVD) risk.2 The ASCVD risk calculator considers age, cholesterol level, and blood pressure. The ACC/AHA guideline suggests prescribing statins such as atorvastatin or rosuvastatin to any person aged 40-75 years whose 10-year risk for developing CVD is >7.5%.7 A patient self-administered risk calculator is also available.2
Prescribing statins: General recommendations
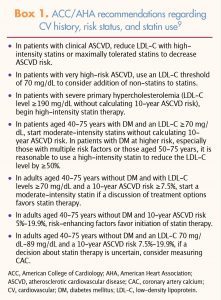 The 2018 ACC/AHA guidelines focus more on intensity of statin therapy and less on LDL-C goals and use of non-statin lipid-lowering agents. More specific recommendations regarding statin dosing depend on a person’s history and CVD risk status (Box 1).9
The 2018 ACC/AHA guidelines focus more on intensity of statin therapy and less on LDL-C goals and use of non-statin lipid-lowering agents. More specific recommendations regarding statin dosing depend on a person’s history and CVD risk status (Box 1).9
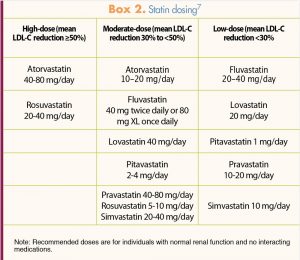
The ACC/AHA recommendations for statins for most individuals involve starting with the appropriate dosage; no evidence supports the previous recommendation to start low and titrate the dosage upward. In the U.S., seven statins are available to treat high cholesterol or prevent cardiovascular events. Box 2 lists these statins and the dosing for each category (high, moderate, low) if applicable.7
Along with prescribing statins when indicated, HCPs should recommend lifestyle changes such as following a heart-healthy diet, getting regular exercise, and maintaining an appropriate weight. Despite the lifestyle interventions and a course of statin therapy, some women may find that they do not tolerate statins or that they fall into one of the following groups: patients who fail to meet LDL-C goals despite maximally tolerated statin therapy, those with recurrent CV events despite maximally tolerated statin therapy, those with significant co-morbidities or high 10-year risk, or those with familial hypercholesterolemia (FH).7
Before starting a woman on a statin, HCPs should evaluate her use of other medications that might interact adversely with a statin.7 In addition, HCPs should check her baseline liver function (aminotransferase levels) and kidney function and assess for and document any pre-existing muscle symptoms. Checking a baseline creatine kinase in women at increased risk for myopathy is suggested.7 Women eligible to start a statin regimen should undergo a fasting lipid panel (TC, HDL-C, calculated LDL-C, triglycerides) at baseline, repeated in 4-12 weeks after initiation or dose adjustment and every 3-12 months as indicated.7
Conclusion
Cardiovascular disease is a serious health concern for women. Current guidelines indicate that all adults should be evaluated for CV risk and, if eligible, should receive statin therapy as primary prevention against CVD. Recent reports of statins’ benefits in primary and secondary prevention of CVD support their use. The statin should be dosed based on a woman’s CV risk, rather than titrating it to specific cholesterol targets. Statins lower levels of atherogenic lipoproteins and reduce CV event-related morbidity and mortality. In most individuals, the benefits of statins outweigh the risks.
- Garcia M, Mulvagh SL, Mertz CN, et al. Cardiovascular disease in women: clinical perspectives. Circ Res. 2016;118(8):1273-1293.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/ AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/ NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1046-e1081.
- ACOG Committee Opinion No. 755: Well-woman visit. Obstet Gynecol. 2018;132(4):e181-e186.
- Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67-e492.
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/ AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934.
- American College of Cardiology. Study Shows New Cholesterol Guideline Has Potential to Increase Eligibility For Statin Therapy. ACC News Story. Mar. 19, 2014. acc.org/latest-in-cardiology/articles/2014/03/19/16/53/study-shows-new-cholesterol-guideline-has-potential-to-increase-eligibility-for-statin-therapy
- Lloyd-Jones DM, Morris PB, Ballantyne CM, et al. 2017 focused update of the 2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology Task Force on Clinical Expert Consensus Decision Pathways. J Am Coll Cardiol. 2017;70(14):1785-1822.
- Boekholdt SM, Hovingh GK, Mora S, et al. Very low levels of atherogenic lipoproteins and the risk for cardiovascular events: a meta-analysis of statin trials. J Am Coll Cardiol. 2014;64(5):485-494.
- Rubenfire M. 2018 ACC/AHA Multisociety Guideline on the Management of Blood Cholesterol. November 2018. acc.org/latest-in-cardiology/ten-points-to-remember/2018/11/09/14/28/2018-guideline-on-management-of-blood-cholesterol
- Lee S, Cannon CP. Combination lipid-lowering therapies for the prevention of recurrent cardiovascular events. Curr Cardiol Rep. 2018;20(7):55.
- Rosenson RS, Hegele RA, Fazio S, Cannon CP. The evolving future of PCSK9 inhibitors. J Am Coll Cardiol. 2018;72(3):314-329.