
The U.S. Medical Eligibility Criteria for Contraceptive Use, 2016 (MEC)1 and the U.S. Selected Practice Recommendations for Contraceptive Use, 2016 (SPR)2 were both released to the public on July 29, 2016. The MEC provides guidance to healthcare providers (HCPs) regarding safe use of contraceptive methods by individuals with certain personal characteristics (e.g., age, smoking status, postpartum status) or medical conditions (e.g., hypertension, diabetes, headaches). The SPR, a companion document to the MEC, provides guidance for common contraceptive management topics such as how to be reasonably certain that a woman is not pregnant, when to start contraception, which exams and tests are medically indicated prior to starting a contraceptive method, what type of follow-up is needed, and how problems should be managed.
The first edition of the MEC was published in 20103 and the first edition of the SPR, in 2013.4 The 2016 updates were made after a thorough review of the scientific evidence and consultation with national experts. A summary of the MEC changes since 2010 is provided in Appendix A of the 2016 edition and a summary of the SPR changes since 2013 appears on page 2 of the 2016 SPR.1, 2
MEC updates
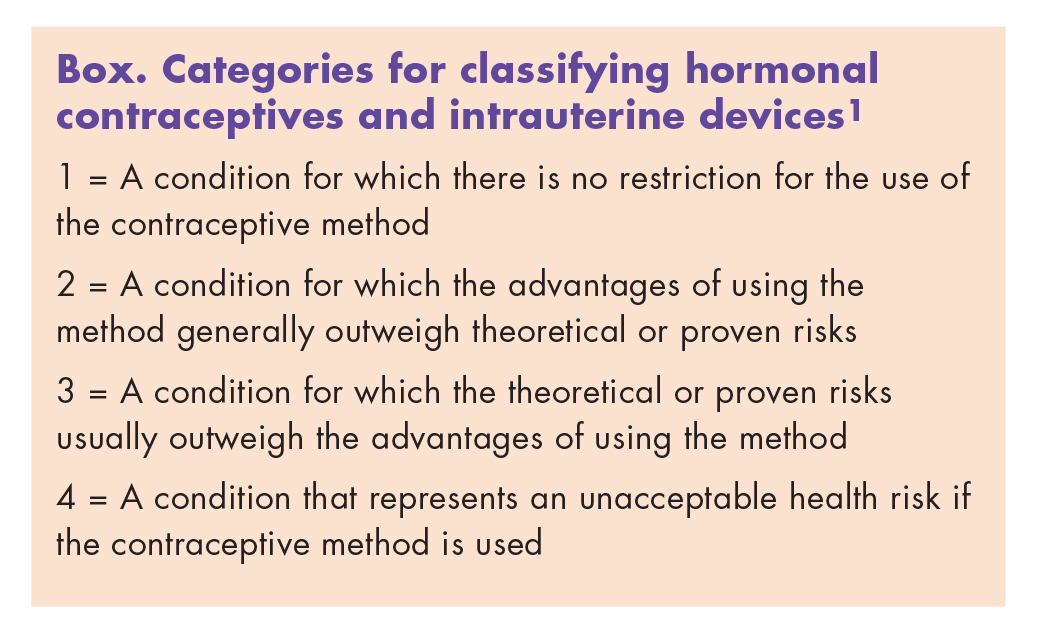
The 2016 MEC provides more than 1,800 recommendations for more than 60 personal characteristics and medical conditions.1 As in the 2010 edition, the 2016 MEC continues to use four categories of medical eligibility to help HCPs assess the safety of a particular contraceptive method for persons with specific personal characteristics or medical conditions (Box). HCPs are reminded that although the MEC recommendations provide guidance, individual circumstances should always be considered in contraceptive method counseling and decisions. Take-home messages in the 2016 MEC remain the same as those in the 2010 edition:
{kind=link}
• Most women can safely use most contraceptives.
• Women with medical conditions associated with an increased risk for adverse health events as a result of pregnancy need highly effective contraception for reproductive life planning.
• Women, men, and couples should be informed of the full range of methods to decide what will be best for them.
• Use of the MEC can help HCPs decrease barriers to choosing safe and effective contraceptive methods.
New recommendations
New to the 2016 MEC are recommendations for women with multiple sclerosis (MS) or cystic fibrosis (CF) and for women taking selective serotonin reuptake inhibitors (SSRIs) or St. John’s wort. Ulipristal acetate (UPA) has been added to the recommendations on emergency contraception (EC).
Multiple sclerosis
HCPs should check the MS subsection of the Neurologic Conditions section of each appendix. In Appendix C, Classifications for Progestin-Only Contraceptives (POCs), depot medroxyprogesterone acetate (DMPA) is listed in category 2 for women with MS, with the comment that these women’s bone health may be compromised due to disease- related immobility and use of corticosteroids. Use of DMPA, which has been associated with small changes in BMD, might be of concern in this patient population. The other POCs, the subdermal implant and progestin-only pills (POPs), are listed in category 1 for women with MS. In Appendix D, Classifications for Combined Hormonal Contraceptives (CHCs), CHCs are listed in category 3 for women with MS who have prolonged immobility and in category 1 for women with MS who do not have prolonged immobility. Of note, although no data suggest an increased risk for venous thromboembolism (VTE) in women with MS using CHCs, these women are at overall higher risk than unaffected women for VTE.
Cystic fibrosis
HCPs should check the CF subsection of the Respiratory Conditions section of each appendix. CF is described as a condition associated with an increased risk for adverse health events as a result of pregnancy. Certain drugs used to treat CF (e.g., lumacaftor) might reduce the effectiveness of hormonal contraceptives, including oral, injectable, transdermal, and implantable contraceptives. In Appendix C, Classifications for POCs, DMPA is listed in category 2 for women with CF, with the comment that these women have a higher prevalence of osteopenia, osteoporosis, and fragility fractures than the general population. Use of DMPA, which has been associated with small changes in BMD, might be of concern in this patient population. The other POCs in women with CF are listed in category 1.
Selective serotonin reuptake inhibitors
HCPs should check the Drug Interactions section in each appendix for specific information about this drugclass. In Appendix A, SSRIs are listed in category 1 for all contraceptives. Available data, albeit limited, show no decrease in the effectiveness of hormonal contraceptives in SSRI users. Likewise, available data show no difference in the effectiveness or in the adverse effects of SSRIs in women using hormonal contraceptives versus those not using them. The comments sections of Appendix C and Appendix D note that drugs that are inhibitors of CYP3A4 or CYP2C9 have the potential, at least in theory, to raise levels of contraceptive steroids, which might increase adverse events. The SSRI fluvoxamine is known to be a moderate inhibitor of both CYP3A4 and CYP2C9; however, no clinical or pharmacokinetic studies were identified to explore these potential drug–drug interactions.
St. John’s wort
HCPs should check the Drug Interactions section in each appendix for information about this herbal product. In Appendix A, St. John’s wort is listed in category 1 for intrauterine devices (IUDs) and DMPA, and in category 2 for the implant, POPs, and CHCs. With regard to the implant, POPs, and CHCs, as noted in Appendix C and Appendix D, limited available data raise concern that St. John’s wort might decrease the effectiveness of hormonal contraceptives by increasing the metabolism of estrogen and progestins. Interactions may be dependent on the dose of St. John’s wort. Also, the concentration of active ingredients in St. John’s wort products may vary. Any potential impact of this herbal product on the contraceptive effectiveness of DMPA is less likely than with the other POCs because of the higher dose of progestin.
Ulipristal acetate
HCPs should check Appendix J, Classifications for Emergency Contraception, for more information about UPA, which has been added to the EC appendix. Like levonorgestrel (LNG) and combined oral contraceptives (COCs) used for EC, UPA is listed in category 2 for women with a history of severe cardiovascular disease, severe liver disease, or obesity, and in those who use a CYP3A4 inducer (e.g., bosentan, carbamazepine, felbamate, griseofulvin, oxcarbazepine, phenytoin, rifampin, St. John’s wort, topiramate, efavirenz, lumacaftor). Of note, for women who are obese or who use strong CYP3A4 inducers, UPA, LNG, and COCs used for EC are listed in category 2 because of possibly reduced effectiveness. There are no personal characteristics or medical conditions that place UPA, LNG, or COCs used for EC in category 3 or 4.
Women who are breastfeeding and have taken UPA are advised to express and discard breast milk for 24 hours after taking the medication. This recommendation has been made because UPA is excreted in breast milk, with highest concentrations in the first 24 hours.
Other MEC revisions
Revisions to recommendations have been made for postpartum and breastfeeding women, as well as for several medical conditions. The revisions to recommendations for postpartum and breastfeeding women include those presented in the 2011 CDC revised recommendations for these populations related to use of the IUD, POCs, and CHCs.5 Appendix B, Classifications for IUDs, includes changes for women with gestational trophoblastic disease, HIV infection, and certain factors related to sexually transmitted infections. Appendix D, Classifications for CHCs, includes changes for women with migraines, superficial venous disease, or known dyslipidemias, and for women on antiretroviral therapy.
SPR updates
As in the 2013 edition, the 2016 SPR provides information organized by contraceptive method.2 Charts and algorithms are included in appendices that summarize guidance across all methods for when to start, examinations and tests that are needed, routine followup, and management of bleeding irregularities. SPR updates are consistent with changes in the 2016 MEC. Take-home messages in the 2016 SPR remain the same as in the 2013 edition:
• Most women can start most methods anytime.
• Few, if any, exams or tests are needed.
• Routine follow-up is generally not required.
• Regular contraception should be started after emergency contraception.
• Anticipatory counseling for potential contraceptive-related bleeding changes and proper management are important.
• Use of the SPR can help HCPs decrease medical barriers to accessing and using contraception.
New recommendation: use of medications to ease IUD insertion
Misoprostol is not recommended for routine use before IUD insertion but might be helpful in some circumstances—for example, in a woman with a recent failed insertion. A paracervical block with lidocaine might reduce pain during IUD insertion.
Updated recommendation: when to start regular contraception after taking UPA
Under ideal circumstances, women should start or resume a hormonal contraceptive method no sooner than 5 days after taking UPA because of a risk that hormonal contraceptives might decrease the effectiveness of UPA. However, if the chosen hormonal method would require an additional visit to an HCP (e.g., DMPA, implant, IUD), the risk of reduced effectiveness needs to be weighed against the risk that a regular contraceptive method might not be started. Women who have taken UPA should abstain from sexual intercourse or use a barrier method for 7 days after starting or resuming regular contraception or until the next menses, whichever comes first. Any nonhormonal contraceptive method can be started immediately after taking UPA.
Useful tools for HCPs
The CDC provides a variety of useful tools and aids to facilitate use of the MEC and SPR in clinical practice. The summary MEC chart has been updated, as has the MEC and SPR Smartphone app. Printable PDF versions of When to Start Contraceptive Methods and Routine Follow-up and What to Do If Late, Missed, or Delayed CHC are available.
Beth Kelsey is Assistant Professor and DNP Program Director at the School of Nursing, Ball State University, in Muncie, Indiana. She is editor-in-chief of Women’s Healthcare: A Clinical Journal for NPs and Publication Coordinator for NPWH. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
1. Centers for Disease Control and Prevention (CDC). U.S. Medical Eligibility Criteria for Contraceptive Use, 2016. July 29, 2016.
2. CDC. U.S. Selected Practice Recommendations for Contraceptive Use, 2016. July 29, 2016.
3. CDC. U.S. medical eligibility criteria for contraceptive use, 2010. June 18, 2010.
4. CDC. U.S. selected practice recommendations for contraceptive use, 2013. MMWR. 2013;62(RR-5):1-46.
5. CDC. Update to CDC’s U.S. medical eligibility criteria for the use of contraceptive methods, 2010: revised recommendations for the use of contraceptive methods during the postpartum period. MMWR. 2011;60(26):878-883.