
Vasomotor symptoms (VMS), including hot flashes and night sweats, are very common in women undergoing menopause.1,2 These symptoms typically result from the alteration of the hypothalamus-pituitary-ovarian-uterine axis as the body undergoes perimenopausal processes such as ovarian aging, hormone fluctuations, decreased estrogen levels, irregular menstrual cycles and cessation.3,4 As a result, 75% of women transitioning naturally and the majority of women with medically induced menopause experience VMS.4,5 VMS also can be accompanied by a variety of other symptoms such as changes in mood, cognition, sleep, and vaginal dryness, headaches, and decreased libido.6,7 These can have a compounding or clustering effect, negatively impacting quality of life.5,6,8 Although hormone therapy (HT), selective serotonin reuptake inhibitors (SSRIs), and serotonin and norepinephrine reuptake inhibitors (SNRIs) are clinically standardized treatments, many women seek alternatives with fewer adverse side effects.9 Among the options are complementary and integrative health (CIH) alternatives such as acupuncture, homeopathy, mind-body techniques such as meditation, mindfulness, yoga, biofeedback, and guided imagery, and dietary supplements.9 This article reviews current knowledge about the efficacy and safety of available dietary supplements to alleviate VMS in menopausal women and implications for clinical practice.
Clinical treatment guidelines
In 2011, the American Association of Clinical Endocrinologists released guidelines for the diagnosis and treatment of VMS.10 Three years later, the American College of Obstetricians and Gynecologists and the North American Menopause Society (NAMS) published clinical guidelines and recommendations for clinical care of menopausal women.11,12 While dated, these guidelines may still be directing clinical practice. The most recent guidance comes from NAMS’ 2022 hormone therapy position statement, which is endorsed by multiple international and national menopause and women’s health associations. A summary of current clinical recommendations for VMS management is provided here.13
The first line of treatment for VMS is HT with or without progestin, depending on whether the woman has an intact uterus.10–12 Due to health risks such as cancer (ie, endometrial, breast, uterine, colon), thrombolytic events, and cardiovascular events, HT should be given at the lowest dose and for the shortest period to alleviate symptoms.10–12 Clinical guidelines for nonhormonal treatments include SSRIs, clonidine, gabapentin, and SNRIs.10–12 Side effects of these nonhormonal treatments include nausea, dry mouth, shakiness, and dizziness.11 Empiric data to support the use of CIH supplements (ie, phytoestrogens, herbal supplements, vitamins, and minerals) is lacking. For now, none of the guidelines support the use of CIH supplements. However, it is important to note that studies investigating CIH supplement safety and efficacy are ongoing.
CIH supplements
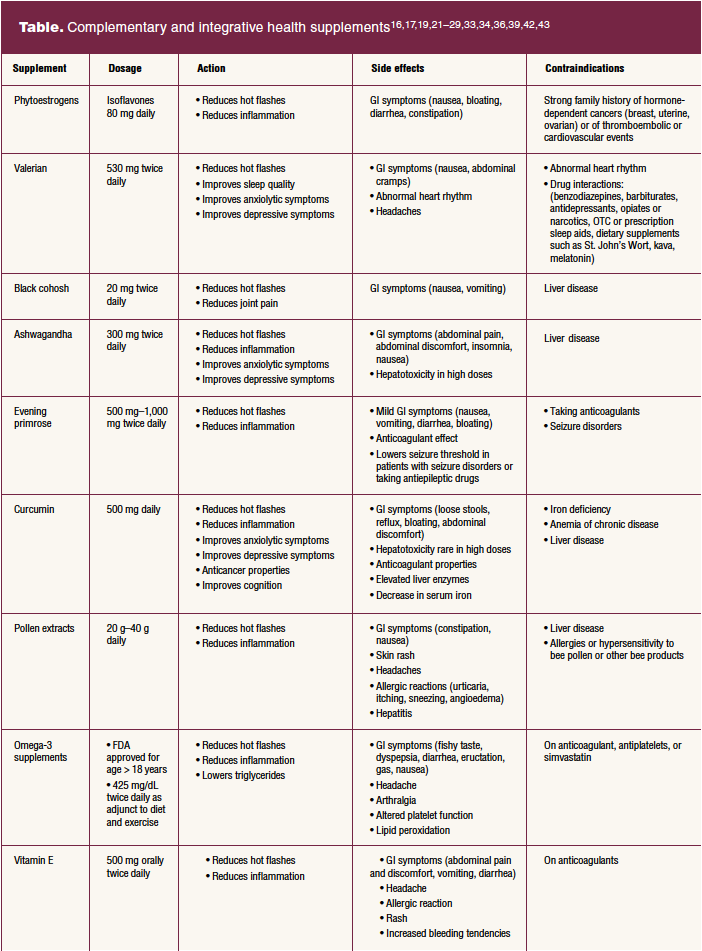
The National Center for Complementary and Integrative Health states that while HT is the most effective treatment for VMS, there are multiple health concerns regarding their use (eg, cancers, thrombolytic events, coronary events).14 In the Woman’s Health Initiative released in 2002, findings from two large, randomized HT trials showed the risks of HT outweigh the benefits.13 Since that time, reanalysis of these data and information from other trials have reduced many of the safety concerns. Based on this information, the 2022 NAMS guidelines state that the benefits of HT outweigh the risks for symptomatic women younger than age 60 or within 10 years of menopause who have no contraindications.13 These guidelines also state that although the benefit-risk ratio may be less favorable, women older than 60 or more than 10 years from menopause onset with persistent VMS affecting quality of life can continue HT based on shared decision making and careful follow-up.13 Due to remaining concerns about health risks and unwanted side effects when taking HT, there are women and healthcare providers opting for a more integrative approach to individualized care and seeking alternative methods for the treatment of VMS.14 Data suggest that CIH supplements may aid in alleviating VMS among menopausal women.15–40 These CIH supplements are discussed here and in the Table.

Phytoestrogens
Phytoestrogens are the most frequently used alternative products for VMS.15–18 Found in plants, fruits, or vegetables, one major class of phytoestrogens is isoflavones.15–18 Isoflavones can be found in soybeans and soy products.9,15–18 Phytoestrogens have chemical structures that resemble estradiol and have estrogenic effects. 9,15–18 Recent studies suggest that these estrogenic qualities may have positive effects for the treatment of VMS.15–18 Epidemiologic studies show that women in Asian countries, such as China and Japan, have a much lower incidence of VMS compared to women in Western countries, such as the United States, possibly due to a higher soy intake.16,17 In a meta-analysis of 15 high-quality randomized controlled trials, hot flashes were reduced in participants taking soy isoflavones tablets or capsules ranging from 5 mg to 100 mg when compared to the use of a placebo.17 Due to their natural estrogenic effects, there are safety concerns with phytoestrogens such as higher risk for cancer (eg, breast, endometrial, uterine, ovarian, colon), thromboembolic events, and/or cardiovascular events that warrant further studies.18 Phytoestrogens have minimal side effects and can be obtained by adding soy-rich foods to a balanced diet.16–18

Valerian
Valerian (Valeriana officinalis), also known as cat grass, is a widely used phytoestrogenic herb with sedative and/or anxiolytic effects.19,20 It contains components that act on the central nervous system, aiding relaxation and improved sleep quality in menopausal women.20 Studies indicate that valerian may reduce VMS as well as anxiety and depressive symptoms.19,20 In a triple-blind randomized clinical trial, 64 menopausal women with VMS received either valerian capsules (530 mg twice daily) or placebo.21 After 2 months, the valerian group reported a reduction in VMS as compared to the placebo group.21 The results of this study suggest that valerian may be a potential approach to alleviating VMS among menopausal women.21 While no side effects were reported in this study, other studies have reported gastrointestinal (GI) symptoms such as nausea and abdominal cramps.21,22
Black cohosh
Black cohosh (Cimicifuga racemosa or Actaea racemosa) is a perennial plant and the most widely studied botanical used to treat VMS.18 Of the 13,096 menopausal women treated with tablets of black cohosh ranging from 8 mg to 128 mg in a 35-study meta-analysis, a reduction in VMS was seen after 4 weeks.23 Sleeping difficulties and anxiety also were reduced.23 Black cohosh demonstrates dopaminergic, serotonergic, and GABAergic effects that aid in addressing hot flashes and assisting with thermoregulation, mood, and sleep.9,20,23 Treatment with black cohosh is generally well tolerated with few to no side effects other than some reports of GI symptoms such as nausea and vomiting.23 In rare cases, a concern with long-term use of black cohosh is hepatotoxicity.9,24 However, other studies report no significant changes in liver function parameters.23 Data indicate that black cohosh is a relatively safe supplement, but caution should be taken due to the variety of different dosages on the market.10,23

Ashwagandha
Ashwagandha (Withania somnifera) has been used in Ayurvedic medicine for thousands of years to enhance longevity, improve overall health, and to treat stress and anxiety.25,26 Ashwagandha, believed to raise estradiol levels through its antioxidant effects, is known for its calming and mood-enhancing abilities.25,26 Studies indicate that ashwagandha may improve VMS and mood in menopausal women.25,26 In an 8-week, randomized, double-blind, placebo-controlled study, 100 women with menopausal symptoms were placed into two groups, an ashwagandha group and a placebo group.25 Results of the study showed that women given ashwagandha 300 mg capsules twice daily experienced improvements in VMS after 8 weeks.25 More long-term studies are required to examine the safety and efficacy of ashwagandha treatment for VMS.25 Side effects reported were mild (ie, abdominal pain, abdominal discomfort, nausea, insomnia).25,26 Long-term use of ashwagandha has been linked to hepatotoxicity.27

Curcumin
Curcumin (Curcuma longa) is a polyphenolic component of the turmeric spice used for centuries for its anticancer, anti-inflammatory, and antioxidant properties.28,29 Curcumin is recognized worldwide for multiple potential health benefits, and recent studies show positive outcomes for its use in alleviating VMS in menopausal women.28 In an 8-week, triple-blind randomized controlled trial among 81 menopausal women, reduction in hot flashes was seen in the curcumin group (taking 500 mg capsules twice daily) after 4 weeks compared to the placebo group.28 The setbacks with taking a curcumin supplement are poor absorption, rapid metabolism, and rapid elimination.30 Piperine, a known bioavailability enhancer, is associated with an increase in the bioavailability of curcumin and has been added to various oral curcumin supplements.30 Curcumin has been approved by the US Food and Drug Administration and is available in many forms (eg, capsules, tablets, ointments, powders).30 Minimal side effects have been reported such as GI symptoms (ie, nausea, diarrhea, yellow stool), headache, and rash.31 Recent concerns of hepatotoxicity have been linked to curcumin.31 Anemia and iron deficiency have been linked to curcumin intake.32 Overall, this appears to be a relatively safe supplement, although no long-term safety studies have been done.32
Evening primrose
Evening primrose (Oenothera biennis) is a botanical with anti-inflammatory properties.33,34 It contains high levels of essential fatty acids such as omega-6 fatty acids and gamma-linolenic acid.33,34 For many years, Native Americans utilized the anti-inflammatory effects of evening primrose for dermal treatments, GI issues, and sore throats.33,34 In an 8-week randomized controlled trial of evening primrose among 170 menopausal women, improvements in night sweats were reported in the evening primrose group (taking 1,000 mg capsules daily) compared to the placebo group. Hot flashes remained unchanged.33 However, other investigators have found menopausal women taking 1,000 mg capsules of evening primrose daily experience less severe VMS and improved quality of life.18,33,34 Side effects of evening primrose include mild GI symptoms (ie, nausea, vomiting, diarrhea, bloating) and lowering the seizure threshold in patients with seizure disorders or taking antiepileptic drugs.30 Evening primrose is contraindicated in women taking blood thinners due to its anticoagulant effect.20,30
Pollen extracts
Pollen extracts from the grass (Poaceae) family including rye (Secale cereale) have been shown to alleviate the symptoms of menopause.36 In a randomized controlled trial among 54 menopausal women, intervention participants were given two tablets every morning with 40 mg of pure pollen extract (GC Fem), and 120 mg of a combined pollen and pistil extract (PI 82) per tablet.36 The intervention group reported a decrease in hot flashes over a 3-month period.36 At follow-up, participants who received a second course of pollen extracts had additional positive effects over and above the original study.36 Although the mechanism of action of pollen extracts is yet to be elucidated, the effects are believed to be due to their strong antioxidant power.36 For safety reasons, more long-term studies are warranted.36
Omega-3 fatty acids
Omega-3 fatty acids are polyunsaturated fatty acids (PUFAs) containing alpha-linolenic acid, eicosatetraenoic acid, and docosahexaenoic acid.37,38 Omega-3 fatty acids are found in fish (eg, sardines, tuna, salmon, halibut, other fish), some plants (ie, green leafy vegetables), seeds, nuts, and beans.37,38 PUFAs are known for their anti-inflammatory and triglycerides-decreasing effects as well as lowering risk for chronic diseases such as heart disease, cancer, and arthritis when ingested.37,38 There has been speculation that omega-3 supplements can aid alleviating VMS.39 In a 16-week randomized controlled trial, a group of 86 healthy postmenopausal women were separated into two groups, with one group given two 425 mg omega-3 capsules and one group given two isoflavone capsules containing 54.4 mg of isoflavones per tablet.39 The results showed a reduction in hot flashes in both groups.39 It suggests that omega-3 supplements may aid in reducing hot flashes in menopausal women, but more studies are required to test for efficacy.39 FDA-approved fatty acid supplements (eg, icosapent ethyl, omega-3-acid ethyl esters, omega-3-carboxylic acids, omega-3-acid ethyl esters) are generally safe with mild side effects such as GI symptoms (eg, fishy taste, dyspepsia, diarrhea, eructation, gas, nausea) and arthalgia.37 Omega-3 fatty acids may affect platelet activation, so patients taking anticoagulants and antiplatelets should not use omega-3 supplements.37,38 There has been some concern for adverse effects on wound healing and lipid peroxidation.37,38

Vitamin E
Vitamin E is an essential lipid-soluble antioxidant found in vegetable oils, nuts, seeds, and green leafy vegetables.40 Good sources of vitamin E include sunflower seeds, almonds, peanuts, olive oil, spinach, and broccoli.40 There are some studies that show vitamin E may reduce VMS in menopausal women.28,29 In an 8-week randomized controlled trial among 93 menopausal women, there was a reduction in hot flashes after 4 weeks in the vitamin E group given 200 IU capsules twice daily.28,29 Vitamin E has known anti-inflammatory effects that are believed to be the mechanism for alleviating VMS.28,29 Side effects reported were GI symptoms (ie, abdominal pain and discomfort, vomiting, diarrhea), headache, allergy, and skin rash.28,29 There are concerns that vitamin E toxicity can lead to increased bleeding. Therefore patients on anticoagulants should use caution when taking vitamin E as a supplement.28,29
Implications for clinical practice
Menopause is an individual experience and nurse practitioners can support menopausal women by individualizing care to each woman’s concerns, beliefs, and preferences.10–14,41 Offering menopause counseling that includes discussing changes in physiology, menopause-related symptoms, psychosocial issues, and treatment options facilitates informed decision making.10–14,41 CIH supplements may be a viable option for women who wish to avoid the side effects of or are unable to take HT and nonhormonal prescription medication for VMS. When suggesting over-the-counter (OTC) supplements, it is important to remember that regulation of dietary supplements by the FDA is extremely limited.10–14 The amount, composition, and quality of supplements will vary depending on brand.12 When choosing CIH supplements, contraindications should be assessed and current medications reviewed to ensure that the selected CIH supplement does not result in detrimental interactions.10,12 Potential side effects and dose-related toxicity should be discussed.
It is important to note that phytoestrogens, vitamin E, curcumin, and omega-3 fatty acids may be introduced into the diet via food sources, rather than OTC CIH supplements.16,28,29,37,41 A diet rich in plant-based foods (ie, fruits, vegetables, whole grains, nuts) may aid menopausal women in the self-management of VMS.10–14
Promoting lifestyle modifications may be beneficial for menopausal women with VMS.10–12 For example, although efficacy has not been supported by empiric evidence, some women report relief by avoiding identified triggers such as caffeine and alcohol, drinking cool liquids, using fans and air conditioning, and the layering of light cotton clothing. Nurse practitioners will want to stay apprised of ongoing study findings regarding efficacy and safety of herbal and dietary supplements for management of VMS. As well, they may want to become knowledgeable about other CIH options that women might be considering for VMS so as to provide evidence-based information to aid in decision making.
C. Rene’ Ray is a PhD student at the University of Alabama/University of Alabama in Huntsville Joint Nursing Science Program, and Jennifer R. Bail, PhD, RN, is Assistant Professor at the University of Alabama in Huntsville. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(2):35-41. doi: 10.51256/WHC042335
References
1 Harper JC, Phillips S, Biswakarma R, et al. An online survey of perimenopausal women to determine their attitudes and knowledge of the menopause. Womens Health (Lond). 2022;18:17455057221106890.
2 Willi J, Ehlert U. Symptoms assessed in studies on perimenopausal depression: a narrative review. Sex Reprod Healthc. 2020;26:100559.
3 Perlman B, Kulak D, Goldsmith LT, Weiss G. The etiology of menopause: not just ovarian dysfunction but also a role for the central nervous system. Glob Reprod Health. 2018;3(2):e8.
4 Zhu D, Chung HF, Dobson AJ, et al. Age at natural menopause and risk of incident cardiovascular disease: a pooled analysis of individual patient data. Lancet Public Health. 2019;4(11):e553-e564.
5 Song Z, Jiang R, Li C, et al. Menopausal symptoms and sleep quality in women aged 40-65 years. Biomed Res Int. 2022;2022:2560053.
6 Larroy C, Marin Martin C, Lopez- Picado A, Fernández Arias I. The impact of perimenopausal symptomatology, sociodemographic status and knowledge of menopause on women’s quality of life. Arch Gynecol Obstet. 2020;301(4):1061-1068.
7 Santoro N, Roeca C, Peters BA, Neal- Perry G. The menopause transition: signs, symptoms, and management options. J Clin Endocrinol Metab. 2021;106(1):1-15.
8 Croke LM. ACOG releases clinical guidelines on management of menopausal symptoms. Am Fam Physician. 2014;90(5):338-340.
9 Moore TR, Franks RB, Fox C. Review of efficacy of complementary and alternative medicine treatments for menopausal symptoms. J Midwifery Womens Health. 2017;62(3):286-297.
10 Goodman NF, Cobin RH, Ginzburg SB, et al; American Association of Clinical Endocrinologists. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the diagnosis and treatment of menopause. Endocr Pract. 2011;17 (suppl 6):1-25.
11 ACOG Practice Bulletin no. 141. Management of menopausal symptoms [published correction Obstet Gynecol. 2016;127(1):166; Obstet Gynecol. 2018;131(3):604]. Obstet Gynecol. 2014;123(1):202-216.
12 Shifren JL, Gass MLS; NAMS Recommendations for Clinical Care of Midlife Women Working Group. The North American Menopause Society recommendations for clinical care of midlife women. Menopause. 2014;21(10):1038-1062.
13 The 2022 Hormone Therapy Position Statement of The North American Menopause Society Advisory Panel. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022;29(7):767-794.
14 Johnson A, Roberts L, Elkins G. Complementary and alternative medicine for menopause. J Evid Based Integr Med. 2019;24:2515690X19829380.
15 De Franciscis P, Colacurci N, Riemma G, et al. A nutraceutical approach to menopausal complaints. Medicina (Kaunas). 2019;55(9):544.
16 Chen LR, Ko NY, Chen KH. Isoflavone supplements for menopausal women: a systematic review. Nutrients. 2019;11(11):2649.
17 Chen MN, Lin CC, Liu CF. Efficacy of phytoestrogens for menopausal symptoms: a meta-analysis and systematic review. Climacteric. 2015;18(2):260-269.
18 Rattanatantikul T, Maiprasert M, Sugkraroek P, Bumrungpert A. Efficacy and safety of nutraceutical on menopausal symptoms in post-menopausal women: a randomized, double-blind, placebo-controlled clinical trial. J Diet Suppl. 2022;19(2):168-183.
19 Mirabi P, Mojab F. The effects of valerian root on hot flashes in menopausal women. Iran J Pharm Res. 2013;12(1):217-222.
20 Kenda M, Glavač NK, Nagy M, Sollner Dolenc M, On Behalf Of The Oemonom. Herbal products used in menopause and for gynecological disorders. Molecules. 2021;26(24):7421.
21 Jenabi E, Shobeiri F, Hazavehei SMM, Roshanaei G. The effect of valerian on the severity and frequency of hot flashes: a triple-blind randomized clinical trial. Women Health. 2018;58(3):297-304.
22 Shinjyo N, Waddell G, Green J. Valerian root in treating sleep problems and associated disorders–a systematic review and meta-analysis. J Evid Based Integr Med. 2020;25:2515690X20967323.
23 Castelo-Branco C, Gambacciani M, Cano A, et al. Review & meta-analysis: isopropanolic black cohosh extract iCR for menopausal symptoms – an update on the evidence. Climacteric. 2021;24(2):109-119.
24 Wuttke W, Jarry H, Haunschild J, et al. The non-estrogenic alternative for the treatment of climacteric complaints: black cohosh (Cimicifuga or Actaea racemosa). J Steroid Biochem Mol Biol. 2014;139:302-310.
25 Gopal S, Ajgaonkar A, Kanchi P, et al. Effect of an ashwagandha (Withania Somnifera) root extract on climacteric symptoms in women during perimenopause: a randomized, double-blind, placebo-controlled study. J Obstet Gynaecol Res. 2021;47(12):4414-4425.
26 Salve J, Pate S, Debnath K, Langade D. Adaptogenic and anxiolytic effects of ashwagandha root extract in healthy adults: a double-blind, randomized, placebo-controlled clinical study. Cureus. 2019;11(12):e6466.
27 Björnsson HK, Björnsson ES, Avula B, et al. Ashwagandha-induced liver injury: a case series from Iceland and the US Drug-Induced Liver Injury Network. Liver Int. 2020;40(4):825-829.
28 Ataei-Almanghadim K, Farshbaf-Khalili A, Ostadrahimi AR, et al. The effect of oral capsule of curcumin and vitamin E on the hot flashes and anxiety in postmenopausal women: a triple blind randomised controlled trial. Complement Ther Med. 2020;48:102267.
29 Farshbaf-Khalili A, Ostadrahimi A, Mirghafourvand M, et al. Clinical efficacy of curcumin and vitamin E on inflammatory-oxidative stress biomarkers and primary symptoms of menopause in healthy postmenopausal women: a triple-blind randomized controlled trial. J Nutr Metab. 2022;2022:6339715.
30 Kargozar R, Azizi H, Salari R. A review of effective herbal medicines in controlling menopausal symptoms. Electron Physician. 2017;9(11):5826-5833.
31 Sohal A, Alhankawi D, Sandhu S, Chintanaboina J. Turmeric-induced hepatotoxicity: report of 2 cases. Int Med Case Rep J. 2021;14:849-852.
32 Fadus MC, Lau C, Bikhchandani J, Lynch HT. Curcumin: an age-old anti-inflammatory and anti-neoplastic agent. J Tradit Complement Med. 2016;7(3):339-346.
33 Kazemi F, Masoumi SZ, Shayan A, Oshvandi K. The effect of evening primrose oil capsule on hot flashes and night sweats in postmenopausal women: a single-blind randomized controlled trial. J Menopausal Med. 2021;27(1):8-14.
34 Farzaneh F, Fatehi S, Sohrabi MR, Alizadeh K. The effect of oral evening primrose oil on menopausal hot flashes: a randomized clinical trial. Arch Gynecol Obstet. 2013;288(5):1075-1079.
35 Wood E, Shields BE. Use of complementary alternative medicine and supplementation for skin disease. Cutis. 2021;108(2):78-83.
36 Winther K, Rein E, Hedman C. Femal, a herbal remedy made from pollen extracts, reduces hot flushes and improves quality of life in menopausal women: a randomized, placebo-controlled, parallel study. Climacteric. 2005;8(2):162-170.
37 Gammone MA, Riccioni G, Parrinello G, D’Orazio N. Omega-3 polyunsaturated fatty acids: benefits and endpoints in sport. Nutrients. 2018;11(1):46.
38 Shahidi F, Ambigaipalan P. Omega-3 polyunsaturated fatty acids and their health benefits. Annu Rev Food Sci Technol. 2018;9:345-381.
39 Palacios S, Lilue M, Mejia A, Menendez C. Omega-3 versus isoflavones in the control of vasomotor symptoms in postmenopausal women. Gynecol Endocrinol. 2017;33(12):951-957.
40 Brigelius-Flohé R. Vitamin E research: past, now and future. Free Radic Biol Med. 2021;177:381-390.
41 Tonob D, Melby MK. Broadening our perspectives on complementary and alternative medicine for menopause: a narrative review. Maturitas. 2017;99:79-85.
42 Ferrari A. Soy extract phytoestrogens with high dose of isoflavones for menopausal symptoms. J Obstet Gynaecol Res. 2009;35(6):1083-1090.
43 Pockaj BA, Gallagher JG, Loprinzi CL, et al. Phase III double-blind, randomized, placebo-controlled crossover trial of black cohosh in the management of hot flashes: NCCTG trial N01CC1. J Clin Oncol. 2006;24(18):2836-2841.
Key words: menopausal symptoms, vasomotor, alternative, herbal, complementary medicine