
The expanding role of the nurse practitioner (NP) into subspecialty settings such as reproductive endocrinology and infertility (REI) necessitates acquiring new technical skills that are particular to the subspecialty in question. NPs who enter the field of REI care for many women who need to undergo hysterosalpingography (HSG), a procedure in which radiopaque dye is instilled into the uterus and fallopian tubes to evaluate tubal patency. Because 30%-40% of female infertility is attributable to a tubal factor,1 this procedure is commonly performed. A major downside of the procedure is that it can engender a considerable amount of anxiety and pain,1-5 a concern to NPs providing patient-centered care.
Increased anxiety may heighten pain perception, which may in turn exacerbate anxiety and lead to more pain,2 a vicious cycle that can have an adverse impact on clinical outcomes associated with HSG. Pain experienced during HSG may lead to premature termination of the procedure or to spasm of the fallopian tube(s), which could be misinterpreted as proximal tubal occlusion (PTO).6.7
Researchers have studied various modalities for easing HSG-related anxiety and pain, including use of a warm or cold medium for the dye,8 educational counseling,1 hysterosalpingo-foam sonography,9 NSAIDs,10 a paracervical block,10,11 paracervical analgesic cream, intrauterine analgesic instillation,10 medicinal herbs,12 or rectal indomethacin13—each with mixed success. As such, additional modalities are needed. One innovation in this regard is the use of music therapy. Listening to music distracts patients and can enable them to have a less stressful experience. Music, which is harmless and inexpensive, can decrease physiologic and cognitive manifestations of anxiety.1
The purpose of this quality improvement (QI) project was to evaluate the use of music therapy in improving patients’ experience during HSG. The project aims were (a) to reduce perceived anxiety in women undergoing HSG and (b) to reduce perceived pain in women undergoing HSG. The authors also ascertained the incidence of PTO in each group.
Methodology
This QI project was reviewed by the Duke University Health System Institutional Review Board and was deemed exempt from approval because it did not meet the criteria for research. The project utilized a pre/post-test design with a pre-intervention group and an intervention group. The pre-intervention group included patients undergoing HSG during a 4-week period prior to implementation of music therapy. The intervention group included patients undergoing HSG with music therapy over the subsequent 4 weeks. In both groups, anxiety was measured immediately before and following HSG, whereas pain was measured only following HSG.
The intervention entailed playing soothing music through a Sonos™ speaker during HSG. A Spotify™ playlist was used on a continuous loop and was the same for each patient. Labrague et al14 listed ideal characteristics of therapeutic music: slow, flowing, and non-lyrical, and played primarily with stringed instruments; songs that best matched these characteristics were chosen for the playlist.
Setting and sample
The setting for this project was a large REI center that performs 40-50 HSGs/week. Within this setting, 24 rotating healthcare providers (HCPs), including 22 physicians and 2 NPs, performed HSG. Modalities commonly used for anxiety and pain in this setting included anticipatory guidance, encouraging deep breathing, distraction via conversation, and pausing the procedure to allow for rest.
A convenience sample was utilized and included all patients undergoing HSG from September 2017 through October 2017. Participation was voluntary. Exclusion criteria included non-English speaking patients, deaf patients, and those who took benzodiazepines prior to the procedure. The final sample consisted of 113 participants in the pre-intervention (no music) group and 134 in the intervention (music therapy) group.
Instruments
Data pertaining to participant demographics and PTO incidence were gathered retrospectively via chart review. To assess anxiety, a modified short-form, six question State-Trait Anxiety Inventory™ (STAI-6) was administered to all participants immediately before entering the HSG room and again in the waiting room following the procedure.15 Reliability of the STAI-6 is 0.82.15 Pain perception was assessed via a 100-millimeter visual analog scale (VAS) immediately post-HSG for both groups16; researchers assumed that no one would have baseline pain. Reliability of the VAS tool is 0.94.16
Data collection and analysis
Pre- and post-HSG anxiety scores and post-HSG pain scores were compared between groups using independent samples t-tests. PTO incidence was analyzed via descriptive statistics and chi-square analysis using SPSS version 24.17 Alpha level was set at .05.
Results
Baseline demographics (age, race/ethnicity, body-mass index, previous HSG) were similar between groups. Members of both groups ranged in age from early 20s to mid-40s, and most had not previously undergone HSG (86%-90%). As shown in the Table, both the no-music and music therapy groups experienced decreases in anxiety scores from pre-HSG testing to post-HSG testing; scores in the two groups did not differ significantly at either checkpoint. Likewise, the groups did not differ significantly with respect to mean post-HSG pain score. Five participants in the no-music group (10.6%) and five in the music therapy group (11.1%) had bilateral PTO on HSG (P = .942). HSGs yielded abnormal results in 47 women (42%) in the no-music group and in 43 women (32.1%) in the music therapy group.
Table. STAI scores and VAS pain scores
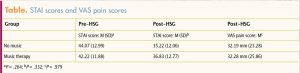
HSG, hysterosalpingography; M, mean; SD, standard deviation; STAI, State-Trait Anxiety Inventory; VAS, visual analog scale.
Limitations
Limitations of this QI project include the convenience sampling technique employed, self-reporting biases, and challenges imposed by inherent differences in each HCP’s HSG technique. In addition, participants were not permitted to choose their own music samplings, which past studies have suggested might influence results in a favorable way.18,19 Furthermore, music was played to the room, not to individual patient headphones, which might have decreased its therapeutic effectiveness.19 The decision to play to the room was made so that patients would still be able to hear instructions during the procedure. Despite limitations, the team continues to use music therapy during HSG and is considering additional evaluative ways to measure patient impact.
Implications for practice
A major disadvantage of HSG is patient-reported anxiety and pain associated with the procedure, which adversely affects not only their experience but also their cooperation—thereby limiting its utility.20 HSG is frequently performed in REI practices, yet a lack of consensus persists regarding the best modalities for anxiety and pain relief.10 NPs open to patient-centered approaches are likely better prepared to succeed with this procedure. Indeed, it is the primary author’s experience that NPs practicing in REI or other settings where HSG is commonly performed would benefit from knowing the wide breadth of pharmacologic and nonpharmacologic strategies for optimizing patients’ experiences. Findings from this QI project support the existing literature emphasizing a multimodal approach to anxiety and pain relief surrounding HSG.10,21
Findings from previous studies of music as an anxiolytic strongly suggest that it has a favorable effect in reducing patient anxiety.14,18,19 Despite this evidence, music therapy recipients in this study did not report less anxiety or pain. Perhaps women in REI settings may already be experiencing symptoms of depression, anxiety, and/or vulnerability3-5 for which music therapy would not have a measurable impact. Women awaiting HSG have been found to have significantly higher levels of anxiety than those awaiting mammography.2 Infertility can cause chronic distress5 and requires multidimensional psychosocial support to help women through the invasive phases of evaluation. Although the data in the present QI project did not demonstrate a reduction of anxiety and pain, music therapy affects other perceptions such as satisfaction, which would be valuable to measure in the future.
Finally, successful implementation of this evidence-based, NP-led QI project within an REI setting underscores the importance of evidence-based practice within REI. More and more NPs are entering the subspecialty of REI. They continue to enhance their skill repertoire as they become valuable members of the team. Demonstration of successfully implemented QI projects allows the team to endorse future NP-led projects that aim to shape quality care. In addition, because of their holistic training, NPs in this field are in a unique position to advance the care of patients with infertility, especially their psychological well-being.22
Conclusion
In this study, music therapy during HSG did not have a significant effect on the reduction of anxiety or pain levels. When patients face a possible diagnosis of infertility, they may be unlikely to respond to any intervention in this setting. Therefore, HCPs need to provide patient-centered care that is customizable for each unique situation.
Hayley E. Eichlin is a women’s health nurse practitioner at Reproductive Medicine Associates of New Jersey in Marlton. Paul A. Bergh is a founding partner and Lauren Nervi is a family nurse practitioner, both at Reproductive Medicine Associates of New Jersey, Basking Ridge. Eleanor L. Stevenson is Associate Professor at Duke University School of Nursing in Durham, North Carolina. Julie A. Thompson is a Research Associate/Statistical Consultant for Duke University School of Nursing in Durham, North Carolina. The authors state that they do not have a financial interest in or other relationship with any commercial product named in this article.
References
- La Fianza A, Dellafiore C, Travaini D, et al. Effectiveness of a single education and counseling intervention in reducing anxiety in women undergoing hysterosalpingography: a randomized controlled trial. ScientificWorld Journal. 2014:1-7. hindawi.com/journals/tswj/2014/598293/
- Tokmak A, Kokanali MK, Güzel AI, et al. The effect of preprocedure anxiety levels on postprocedure pain scores in women undergoing hysterosalpingography. J Chin Med Assoc. 2015;78(8):481-485.
- Williams M, Green L, Roberts, K. Exploring the needs and expectations of women presenting for hysterosalpingogram examination following a period of subfertility: a qualitative study. Int J Clin Pract. 2010;64(12):1653-1660.
- Angioli R, De Cicco Nardone C, Plotti F, et al. Use of music to reduce anxiety during office hysteroscopy: prospective randomized trial. J Minim Invasive Gynecol. 2014;21(3):454-459.
- Handelzalts JE, Levy S, Peled Y, et al. Information seeking and perceptions of anxiety and pain among women undergoing hysterosalpingography. Eur J Obstet Gynecol Reprod Biol. 2016;202:41-44.
- Atalabi OM, Osinaike BB. Do abnormal findings on hystero-salphingographic examination correlate with intensity of procedure associated pain? Afr J Reprod Health. 2014;18(2):147-151.
- Dun EC, Nezhat CH. Tubal factor infertility: diagnosis and management in the era of assisted reproductive technology. Obstet Gynecol Clin North Am. 2012;39(4):551-566.
- Zhu YY, Mao YZ, Wu WL. Comparison of warm and cold contrast media for hysterosalpingography: a prospective, randomized study. Fertil Steril. 2012;97(6):1405-1409.
- Dreyer K, Out R, Hompes PG, Mijatovic V. Hysterosalpingo-foam sonography, a less painful procedure for tubal patency testing during fertility workup compared with (serial) hysterosalpingography: a randomized controlled trial. Fertil Steril. 2014;102(3):821-825.
- Unlu BS, Yilmazer M, Koken G, et al. Comparison of four different pain relief methods during hysterosalpingography: a randomized controlled study. Pain Res Manag. 2015;20(2):107-111.
- Jain S, Inamdar DB, Majumdar A, Jain DK. Effectiveness of paracervical block for pain relief in women undergoing hysterosalpingography. J Hum Reprod Sci. 2016;9(4):230-235.
- Gharib M, Samani LN, Panah ZE, et al. The effect of valeric on anxiety severity in women undergoing hysterosalpingography. Glob J Health Sci. 2015;7(3):358-363.
- Karaman E, Çim N, Alkis I, et al. Rectal indomethacin use in pain relief during hysterosalpingography: a randomized placebo controlled trial. J Obstet Gynaecol Res. 2016;42(2):195-201.
- Labrague LJ, McEnroe-Petitte DM. Influence of music on preoperative anxiety and physiologic parameters in women undergoing gynecologic surgery. Clin Nurs Res. 2016;25(2):157-173.
- Marteau TM, Bekker H. The development of a six-item short-form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI). Br J Clin Psychol. 1992;31(3):301-306.
- Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken). 2011;(63 suppl 11):S240-S252.
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp; 2016.
- Agwu KK, Okoye IJ. The effect of music on the anxiety levels of patients undergoing hysterosalpingography. 2007;13(2):122-125.
- Johnson B, Raymond S, Goss J. Perioperative music or headsets to decrease anxiety. J Perianesth Nurs. 2012;27(3):146-154.
- Szymusik I, Grzechocińska B, Marianowski P, et al. Factors influencing the severity of pain during hysterosalpingography. Int J Gynaecol Obstet. 2015;129(2):118-122.
- Mak N, Reinders IMA, Slockers SA, et al. The effect of music in gynaecological office procedures on pain, anxiety and satisfaction: a randomized controlled trial. Gynecol Surg. 2017;14(1):14.
- Koroma L, Stewart L. Infertility: evaluation and initial management. J Midwifery Womens Health. 2012;57(6):614-621.