
Minimally invasive office gynecology procedures such as endocervical polypectomy and endometrial biopsy are routinely performed by women’s health nurse practitioners (WHNPs). To ensure patient safety and comfort and to avoid complications, the WHNP must have knowledge of indications and contraindications, as well as skills needed to perform each of these procedure competently and efficiently. WHNP programs provide didactic and clinical instruction for these skills, often in a supervised clinical simulation format. However, the fast-paced clinical setting does not necessarily provide novice WHNPs or WHNP students with an environment conducive to feeling confident when they first perform these office gynecology procedures on their own.1
Simulation learning is a valuable strategy for acquiring skill and confidence in performing clinical procedures. The Institute of Medicine report, To Err is Human: Building a Safer Health System, recommends simulation learning as a means to help prevent errors in the clinical setting.2 Simulation learning provides a controlled, risk-free environment for learners that allows time for adequate practice to acquire skills and confidence.
The purpose of this article is to provide examples of simulation modules that can be used to review and practice the required steps previously learned to promote confidence prior to performing endocervical polypectomy or endometrial biopsy on a patient. The materials used in these simulation modules are readily available outside the clinical learning lab. Novice WHNPs who have not yet performed endocervical polypectomy or endometrial biopsy in clinical practice, WHNPstudents, and even instructors and preceptors for WHNP students, may find these simulation modules helpful. The photographs in this article are screen shots from the simulation modules.
Endocervical polypectomy
Case study presentation
A G4 P2204, 29-year-old female presents to the clinic with this complaint: “I’ve been spotting after sex for the past 2 months.” She denies vaginal discharge or odor. Her last menstrual period occurred 1 week ago and was described as heavy without visible clots. She is married and sexually active with one partner. The vaginal ring is used for contraception. The WHNP performs a speculum examination, which shows a thin, 2-cm-long, red, pedunculated growth protruding from the cervical os. Given the patient’s presenting complaint and physical exam findings, the WHNP thinks that a pathology report will confirm a diagnosis of endocervical polyp.
Indications for procedure
The purpose of an endocervical polypectomy is to remove the pedunculated growth from the cervix and rule out malignancy of the tissue. Although fewer than 5% of all endocervical polyps are malignant, all of them should undergo biopsy.3 Removal is indicated to stop intermittent spotting and bleeding symptoms related to the polyp.4
Diagnosis
The diagnosis in this case is endocervical polyp. The ICD-10 code for endocervical polyp is N84.1. The current procedural terminology (CPT) code for an endocervical polypectomy is 58999.
Procedure directions
Prior to the procedure, the WHNP reviews risks and benefits with the patient and obtains her signature on the consent form. The WHNP confirms any allergies with the patient, especially those related to solutions that may be used to cleanse the cervix. A urine pregnancy test is obtained if the patient is sexually active and premenopausal. Endocervical polypectomy is contraindicated during pregnancy because increased blood flow to the cervix may result in substantial bleeding. The WHNP assists the patient in reclining in the dorsal lithotomy position on the exam table, with both feet placed in the stirrups, provides appropriate draping, and confirms her comfort.
After washing the hands and applying clean gloves, the WHNP inserts an appropriate-size speculum into the vagina and visualizes the cervix with the polyp protruding from the endocervical canal (Photograph 1). A benign endocervical polyp is thin, red, and smooth in appearance.5 Caution to proceed is exercised if the endocervical mass appears thick. Cervical cancer, an endometrial polyp, and uterine fibroids may resemble an endocervical polyp.5
{kind=link}
The WHNP cleans the cervix with povidone iodine or other appropriate antiseptic solution. The WHNP then inserts a small sterile cotton swab just inside the endocervical canal and moves it in a clockwise direction completely around the inside of the canal to confirm the location of the polyp base. If the WHNP cannot locate the polyp base or freely move the swab in the cervical canal, the procedure is halted and the patient is referred to a gynecologist for further evaluation of the endocervix and endometrial cavity with a hysteroscope.
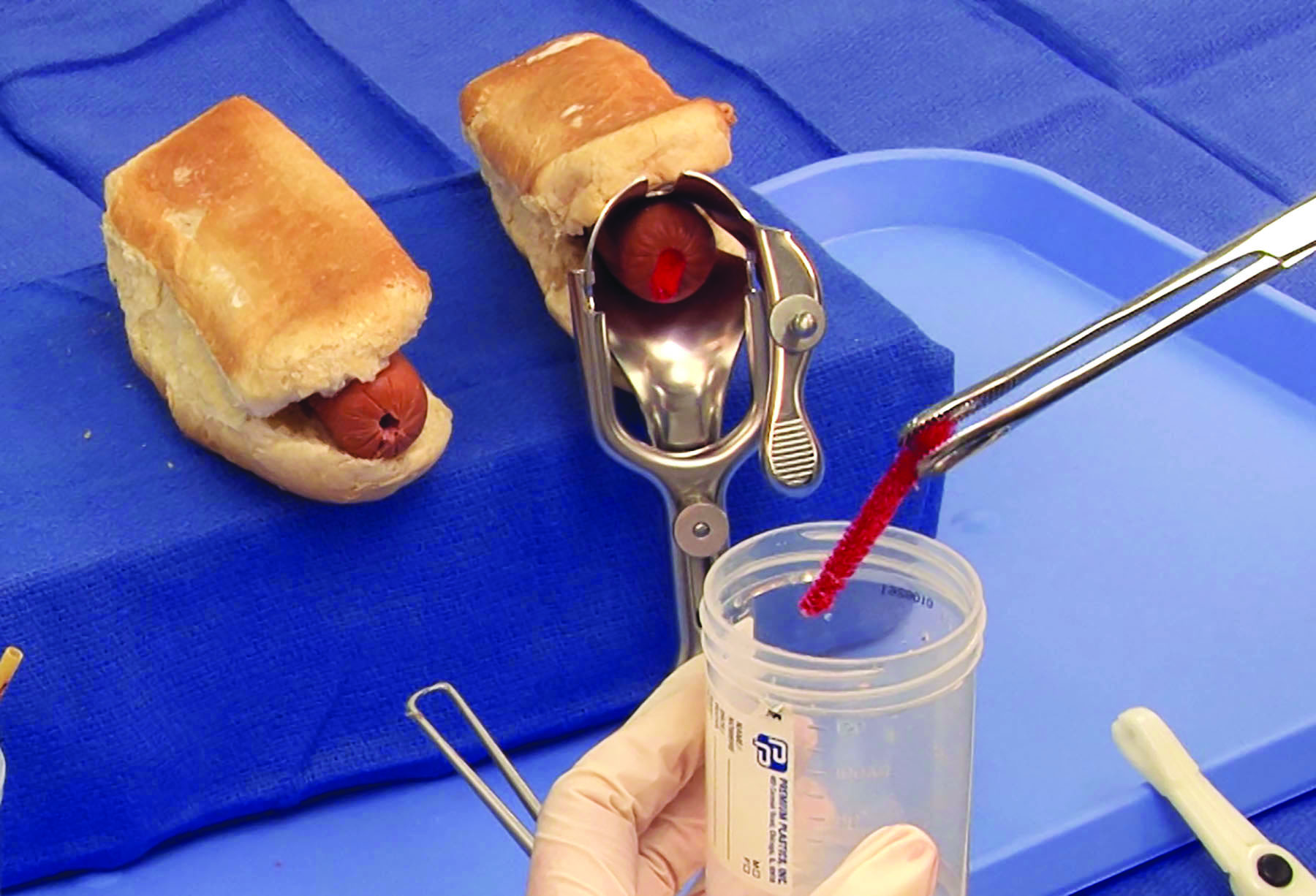
Otherwise, the next step is to securely close a ring forceps around the endocervical polyp as close to the base as possible and twist the polyp in a clockwise direction, applying gentle tension. The WHNP continues twisting the polyp until the base is no longer attached to the cervix. The specimen is then placed in a container of liquid formalin (Photograph 2). If bleeding is observed at the site, the WHNP applies pressure using a large cotton swab. If necessary, a silver nitrate stick or Monsel’s solution can be applied to manage bleeding. The speculum is then gently removed, and the patient is slowly assisted into an upright sitting position, with her stability assessed.
{kind=link}
The WHNP confirms that the patient’s identification information is on the container and that a pathology requisition form is included in the biohazard bag that accompanies the biopsy specimen to the laboratory. The requisition form always includes the patient’s name, second patient identifier, date and time of collection, specimen source, diagnosis, and practitioner’s name.
Post-procedure patient education
The WHNP informs the patient that vaginal spotting/bleeding is not uncommon a few hours after the procedure. A peri-pad is offered to the patient, who is advised to avoid placing anything into the vagina for a few days post-procedure. The patient is asked to notify the WHNP if any of these situations occur: pelvic pain not relieved with a non-steroidal anti-inflammatory drug (NSAID), malodorous vaginal discharge, continuous bright red vaginal bleeding, or fever.6
Description of the simulation
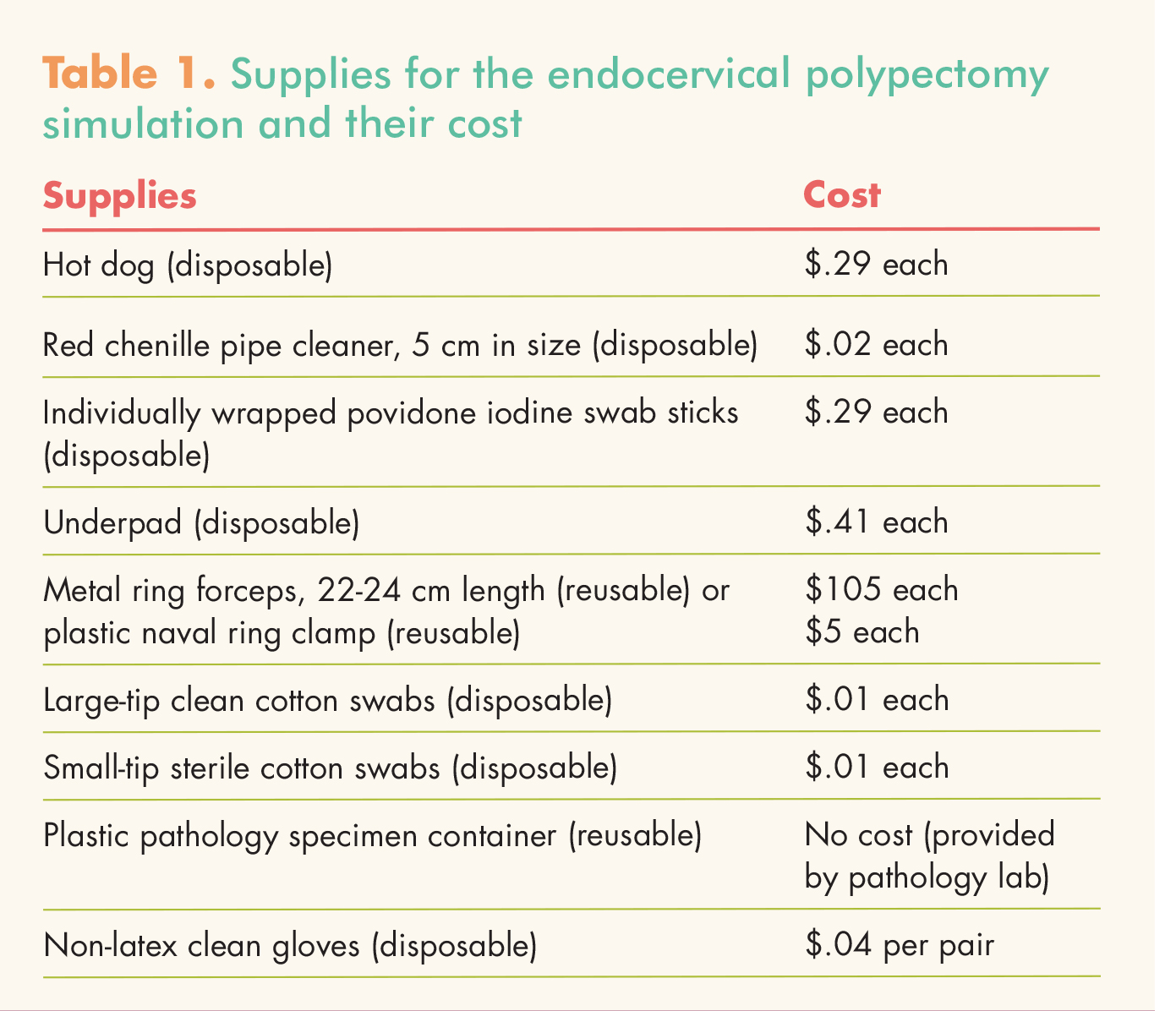
Supplies (Table 1) may be purchased from a medical supplier, a craft store, a grocery store, or an online store. Most supplies are disposable, but some are reusable. Simulation learning is a cost-effective way to practice procedures. This endocervical polypectomy
{kind=link}
simulation can be performed at a cost of about $6.
Step-by-step simulation assembly and video link
Cut off a 5-cm piece of red chenille pipe cleaner. Insert the pipe cleaner into the center of a hot dog, leaving approximately 2-3 cm of it on the outside of the hot dog. Readers can access a video link for the endocervical polypectomy simulation. This video is the intellectual property of the University of Alabama at Birmingham and cannot be shared without request of a license (to do so, please contact the author at aimeeholland@uab.edu). However, NPWH members are encouraged to share the article itself, which contains links to the videos, with their colleagues.
Endometrial biopsy
Case study presentation
A 55-year-old menopausal patient presents to the clinic with this complaint: “My period has come back on. I’ve been spotting and bleeding from my vagina intermittently for the past 3 months.” The woman’s last menstrual period took place when she was 52 years old. The patient, a widow, has not had sexual intercourse in the past 2 years.
Indications for procedure
The purpose of an endometrial biopsy is to rule out endometrial cancer. Based on the American Congress of Obstetricians and Gynecologists’ Committee Opinion Number 557, an endometrial biopsy should be performed for women older than 45 years as a first-line screen for abnormal uterine bleeding (AUB).7 Another indication for an endometrial biopsy is exposure to unopposed estrogen in a woman younger than 45 who experiences persistent AUB after failed medical management.7
Diagnosis
The diagnosis in this case is postmenopausal bleeding. The ICD-10 code for postmenopausal bleeding is N95.0. The CPT code for an endometrial biopsy without cervical dilation is 58100.
Procedure directions
Prior to the procedure, the WHNP reviews risks and benefits with the patient and obtains her signature on the consent form. The WHNP confirms any allergies with the patient, especially those related to solutions that may be used to cleanse the cervix. A urine pregnancy test is obtained if the patient is sexually active and premenopausal. Endometrial biopsy is contraindicated during pregnancy. The WHNP assists the patient in reclining in the dorsal lithotomy position on the exam table, with both feet placed in the stirrups, provides appropriate draping, and confirms her comfort.
After washing the hands and applying clean gloves, the WHNP performs a bimanual exam to determine the position of the uterus and cervix and the presence of any tenderness or masses in the pelvis. The WHNP inserts an appropriate-size speculum into the vagina to visualize the cervix, which is then cleaned with povidone iodine or other appropriate antiseptic solution (Photograph 3). After confirming patency of the cervical os and measuring the depth of the uterus with a uterine sound (i.e., sounding the uterus), the WHNP obtains a sterile endometrial pipelle and inserts it into the cervix and uterus.
{kind=link}
Difficulty inserting the pipelle may be due to a natural curvature in the cervix or uterus. Depending on this curvature, the WHNP may need to use a sterile method to slightly bend the tip of the pipelle in order for it to slide completely into the uterine cavity. The WHNP may need to apply an instrument, such as a tenaculum, a ring forceps, or a long hemostat to the cervix to help straighten the natural curvature of the cervix and uterus, ensuring that the patient is prepared for the use of an additional instrument (Photograph 4).
{kind=link}
Once the pipelle is inserted to the top of the uterine fundus, the WHNP pulls back rapidly on the piston as far as it will go to create suction. The WHNP passes the pipelle in and out between the fundus and internal cervical os 3 or 4 times while continuously turning it a full 360°, rolling it between the thumb and index finger. Endometrial tissue will begin to collect inside the pipelle. Once an acceptable amount of tissue is visualized, the pipelle is removed from the uterus. The WHNP carefully expels the tissue from the pipelle by pushing the piston forward into a plastic container of formalin, and confirms that a sufficient amount of tissue has been collected (Photograph 5). The vaginal speculum is then gently removed. The patient is slowly assisted to an upright sitting position and her stability is assessed.
{kind=link}
The WHNP confirms that the patient’s identification information is on the container and that a pathology requisition form is included in the biohazard bag that accompanies the biopsy specimen to the laboratory. The requisition form always includes the patient’s name, second patient identifier, date and time of collection, specimen source, diagnosis, and practitioner’s name.
Post-procedure patient education
The WHNP informs the patient about the most common symptoms experienced with an endometrial biopsy, which include pelvic pain, vaginal bleeding, and fainting.8 The patient is advised to notify the WHNP if she experiences
uterine cramping lasting longer than 48 hours or not resolved with an NSAID, malodorous vaginal discharge, heavy vaginal bleeding, or fever.6
Description of the simulation
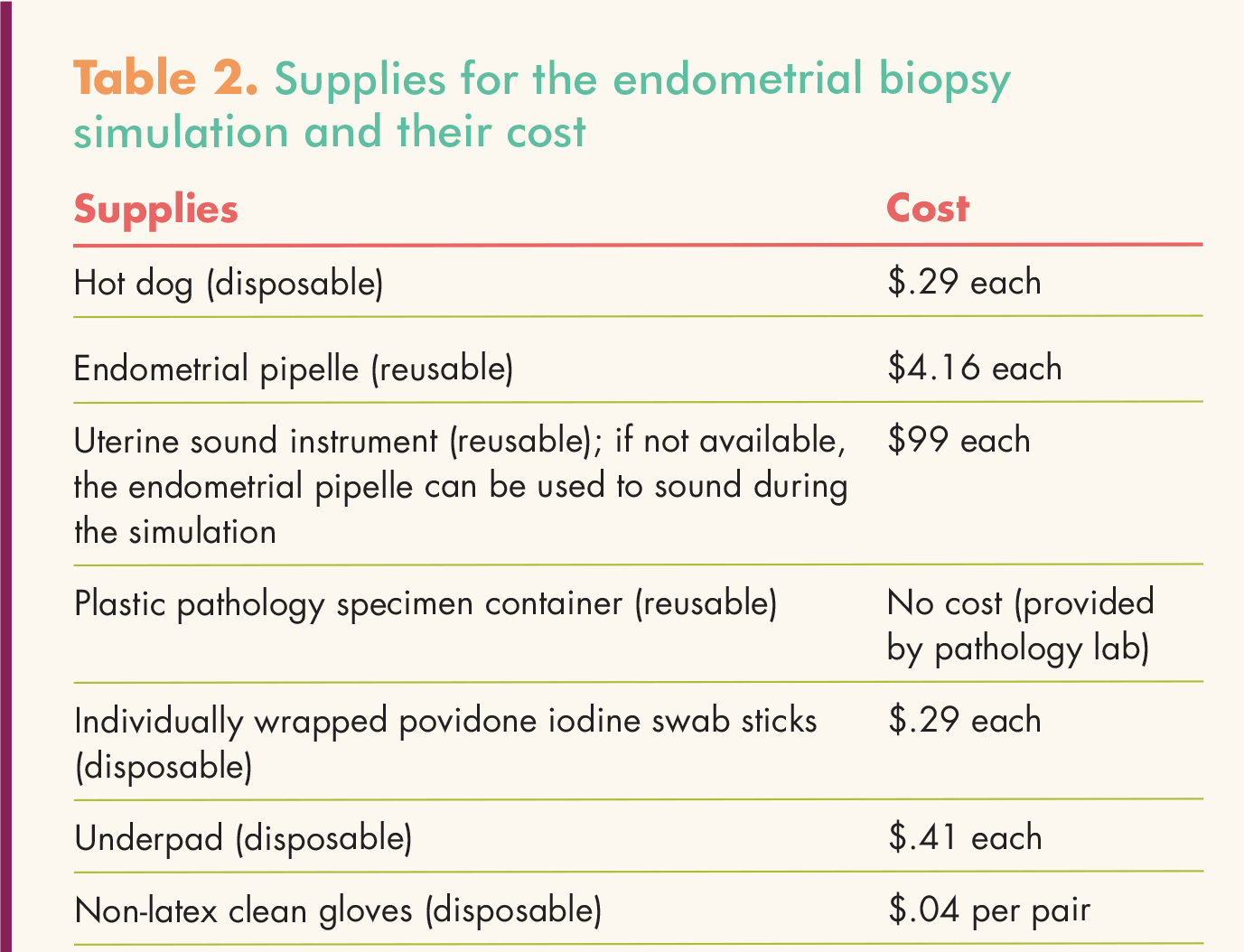
Supplies (Table 2) may be purchased from a medical supplier, a craft store, a grocery store, or an online store. Most supplies are disposable, but some are reusable. Simulation learning is a cost effective way to practice procedures. This simulation endometrial biopsy can be performed at a cost of about $5. Readers can access a video link of the endometrial biopsy simulation. This video is the intellectual property of the University of Alabama at Birmingham and cannot be shared without request of a license (to do so, please contact the author at aimeeholland@uab.edu). However, NPWH members are encouraged to share the article itself, which contains links to the videos, with their colleagues.
{kind=link}
Conclusion
Women’s health nurse practitioners are important performers of minimally invasive gynecology procedures such as endocervical poly pectomy and endometrial biopsy. However, the fast-paced clinical setting may not provide the novice WHNP or WHNP student with an environment conducive to mastering newly learned skills. Simulation learning has educational and clinical benefits to enhance practice.9 In a controlled, simulated environment, individuals can focus on achieving competency, efficiency, and confidence when performing these procedures.9, 10
Aimee Chism Holland is Assistant Professor at the University of Alabama at Birmingham School of Nursing. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article. The author heartily thanks Mr. James Clark, Instructional Design Specialist at the UAB School of Nursing, for recording these procedures for her.
References
1. Nakajima AK, Posner GD. Human Simulation for Women’s Health. New York, NY: Springer Publishing Company; 2012.
2. Kohn LT, Corrigan JM, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Washington, DC: Committee on Quality of Health Care in American, Institute of Medicine; 2000.
3. Beckmann C, Ling F, Herbert W, et al. Obstetrics and Gynecology. 7th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2013.
4. Stewart EA. Endometrial polyps. UpToDate. October 21, 2013.
5. Hoffman BH, Schorge J, Schaffer J, et al. Williams Gynecology. 2nd ed. New York, NY: McGraw Hill; 2012.
6. Sulik S, Heath C. Primary Care Procedures In Women’s Health. New York, NY: Springer Publishing Company; 2010.
7. American Congress of Obstetricians and Gynecologists. ACOG committee opinion no. 557. Management of acute abnormal uterine bleeding in non-pregnant reproductive aged women. Obstet Gynecol. 2013;121(4): 891-896.
8. Blumenthal PD, Berek JS. A Practical Guide to Office Gynecologic Procedures. Philadelphia, PA: Lippincott, Williams & Wilkins; 2013.
9. Cooper S, Cant R, Porter J, et al. Simulation based learning in midwifery education: a systematic review. Women Birth. 2012;25(2):64-78.
10. Nitschmann C, Bartz D, Johnson NR. Gynecologic simulation training increases medical student confidence and interest in women’s health. Teach Learn Med. 2014;26(2):160-163.