
This article provides novice women’s health nurse practitioners (WHNPs) and WHNP students, as well as instructors and preceptors for WHNP students, with detailed information needed to safely, competently, and efficiently perform two vulvar procedures commonly done in outpatient women’s healthcare settings: vulvar biopsy and application of trichloroacetic acid as a treatment for vulvar condylomata acuminata. The author presents two simulation modules that can be used to practice and refine skills for performing these procedures.
Vulvar biopsy and application of trichloroacetic acid (TCA) to treat vulvar condylomata acuminata (genital warts) are two minimally invasive office procedures routinely performed by women’s health nurse practitioners (WHNPs). To ensure patient safety and good outcomes, WHNPs must receive formal education and training prior to performing these procedures. The busy women’s health or primary care clinic is not always an ideal environment for novice WHNPs or WHNP students to practice these types of skills.1
Simulation training offers an opportunity for learners to acquire knowledge, hone skills, and gain confidence. The National League of Nursing promotes simulation training as an effective teaching methodology to prepare nurses for practice.2 The current literature supports simulation-based training with practice as an effective means to achieve patient safety.3 Simulation provides novice WHNPs and WHNP students with an opportunity to practice office gynecology skills in a safe environment conducive to increasing competency and efficiency.4 This article provides these learners, as well as WHNP faculty and preceptors of WHNP students, with simulation modules that can be used to review, practice, and master the steps needed to perform two specific vulvar procedures.
Vulvar biopsy
Case study presentation
A G2 P2002, 69-year-old postmenopausal woman presents to the clinic with this complaint: “I’ve had persistent itching on the left side of my vulva for 3 months.” She denies having vulvar or vaginal bleeding, discharge, or odor. She has been applying over-thecounter (OTC) cream for yeast vaginitis, 1% hydrocortisone cream, and warm compresses to the affected area, with little relief. The WHNP performs a visual examination of the vulva and observes an irregularly shaped, pigmented lesion approximately 3 cm wide on the left side of the vulva. Given the patient’s presenting complaint and the physical exam findings, the WHNP thinks that a pathology report will confirm the presence of vulvar intraepithelial neoplasia (VIN). Until the pathology report is received, vulvar pruritus is documented as the diagnosis in the patient’s health record.
Indication for procedure
The American College of Obstetricians and Gynecologists recommends performing a biopsy for any pigmented lesion on the vulva or for a case involving vulvar symptoms that persist despite topical therapy.5 The purpose of the biopsy is to determine the cause of the symptoms and to rule out malignancy. Biopsy-proven VIN is a risk factor for vulvar cancer.5
Contraindications
No absolute contraindications for vulvar punch biopsy exist; relative contraindications include coagulation disorder, current infection at the biopsy site, allergy to local anesthetic, and inability to comply with wound care.6 If melanoma is suspected, the WHNP should refer the patient to a dermatologist or gynecologist-oncologist to perform the biopsy.
Diagnosis
The diagnosis in this case is vulvar pruritus; the ICD-10 code is L29.2. The CPT code for a vulvar biopsy is 56605.
Procedure directions
Initial steps include reviewing risks and benefits of the procedure with the patient, obtaining a signature on the consent form, and ruling out any allergies associated with antiseptic solutions used for cleansing the vulva. The patient is draped appropriately, assisted into the reclined position on the exam table with both feet in the stirrups, and asked if she is comfortable. Before performing the procedure, the WHNP ensures that a good light source is available.
After washing the hands and applying clean gloves, the WHNP observes the vulvar lesion to identify where to collect the biopsy; the area with the greatest observed changes in texture and
color is chosen. The WHNP cleans the area with povidone iodine or another appropriate antiseptic solution. Using a 22-gauge needle and a tuberculin syringe, the WHNP injects 1-2 mL of 2% lidocaine with epinephrine at the biopsy site. About 2-3 minutes later, the WHNP confirms with the patient that the site is numb by using a sterile cotton swab to lightly touch the area. Using a 3-mm Keyes biopsy punch, the WHNP applies gentle pressure while slowly and steadily twisting the instrument clockwise and counterclockwise until the punch is fully inserted into the pigmented lesion (Photograph 1). The punch is removed and the location of the tissue sample is identified. Using sterile forceps, the WHNP picks up the tissue sample and removes it using sterile scissors (Photograph 2). The WHNP places the specimen into a pathology container with liquid formalin. If bleeding is observed at the site, the WHNP applies pressure using sterile cotton gauze or a cotton swab. Next, the WHNP applies a small amount of antibacterial ointment to the biopsy site and covers it with a bandage.
{kind=link}
{kind=link}
The WHNP confirms that the patient’s identification information is documented on the outside of the container and that a pathology requisition form is included in the biohazard bag that accompanies the biopsy specimen to the laboratory. The requisition form includes the patient’s name, a second patient identifier, date and time of the biopsy collection, specimen source, diagnosis, ICD-10 code, and practitioner’s name.
Post-procedure patient education
The WHNP reassures the patient that slight bleeding at the biopsy site is normal and that minor discomfort may be experienced. The patient is asked to notify the WHNP if she experiences pain unrelieved by use of an OTC nonsteroidal anti-inflammatory drug (NSAID), malodorous or bloody drainage from the biopsy site, or a temperature of 100.5º F or higher.6
Description of the simulation
Supplies (Table 1 ) may be purchased from a medical supplier, a craft store, or a grocery store. Most of the supplies are disposable, but some can be reused. Simulation training is a safe and cost-effective way to practice procedures. This vulvar biopsy simulation can be performed at a cost of about $5.
{kind=link}
Step-by-step simulation assembly and video link
The first step is to cut a small piece (3 cm x 3 cm) of raw calf’s liver with the shiny sheath visible on top. A lesion can be drawn on the liver with a red marker if desired. The liver is dried with the disposable underpad before the lesion is drawn. Readers can access a video link for the vulvar biopsy simulation.*
Trichloroacetic acid treatment for vulvar condylomata acuminata
Case study presentation
A G0 20-year-old woman visits the clinic for the first time. She presents with the complaint, “I have vulvar warts—again,” and asks the WHNP for treatment. She denies having vaginal discharge, itching, or odor. She is single and sexually active with one partner. She uses depot medroxyprogesterone acetate for contraception. She denies ever smoking cigarettes. She also denies receiving the HPV vaccination. The WHNP inspects the patient’s vulva and visualizes a small cluster of condylomata acuminata 2 cm in diameter and two individual warts about 1 cm in diameter each on the right side of the vulva at the 4 o’clock position. No discharge or odor is present. Given the patient’s history of condylomata acuminata, the WHNP discusses treatment options with her and recommends topical treatment with TCA. In addition, the patient is advised to receive the first of three doses of the 9-valent HPV vaccine. The first application of TCA and the first dose of the HPV vaccine are administered at this visit. The WHNP asks the patient to return for a follow-up visit in 1 week and educates her about the importance of undergoing cervical cancer screening when she reaches age 21, along with the importance of routine condom use for sexually transmitted infection prevention.
Indication for procedure
Ninety percent of genital warts are caused by HPV type 6 or 11.7 Genital warts can occur as simple lesions or in clusters. Patients describe them as unattractive, irritating, and itchy. Left untreated, genital warts can disappear within 12-24 months, remain unchanged, or multiply.7 Various treatments can relieve the aesthetic concerns and bothersome symptoms, but no therapy can eradicate the HPV infection from the body.7 Treatment of existing genital warts does not prevent future ones from occurring.
Contraindications
The only absolute contraindication for using TCA is the presence of a hypersensitivity or an allergy to it. TCA should not be used to treat genital warts of the urethra, vagina, cervix, or rectum.
Diagnosis
The diagnosis in this case is anogenital warts. The ICD-10 code is A63.0. Application of TCA is considered simple destruction of vulvar lesions and is billed as a CPT code of 56501.
Treatment procedure directions
Prior to the TCA application, the WHNP discusses risks and benefits of the procedure with the patient and obtains her signature on the consent form. The patient is asked if she has any allergies, especially those related to povidone iodine or TCA. The patient is draped appropriately, assisted into the dorsal lithotomy position on the exam table with both feet placed in the stirrups, and asked if she is comfortable.
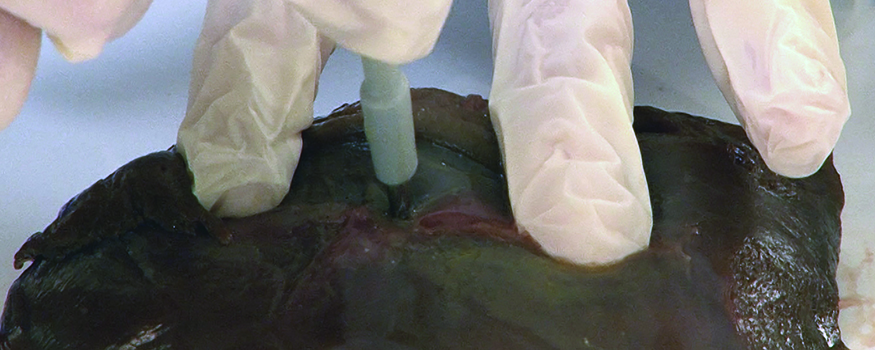
After washing the hands and applying clean gloves, the WHNP inspects the external genitalia to locate the vulvar warts. The area is cleaned with povidone iodine or another appropriate antiseptic solution. Using a small cotton-tip swab, the WHNP applies petroleum jelly to a thin circular area around each wart to prevent the TCA from spreading when it is applied (Photograph 3). In addition,the WHNP can numb the area surrounding the warts with 2% topical lidocaine gel if this product is available in the clinic. The TCA is then applied to the warts using a small cotton-tip swab (Photograph 4 ). The WHNP touches the swab directly to the wart and holds it there until the area blanches. The TCA is allowed to dry completely. The patient’s discomfort level is assessed. If she is experiencing discomfort, then the WHNP applies baking soda to the treated area to help neutralize the acid.7 These steps are repeated until the warts have a frost-like appearance (Photograph 5).
{kind=link}
{kind=link}
{kind=link}
Post-procedure patient education
The WHNP informs the patient about the pain and burning sensation commonly experienced after application of TCA. The patient is advised to use sitz baths, topical lidocaine, cool compresses, and/or oral NSAIDs to help relieve the discomfort. She is advised to wear a small peri-pad for the remainder of the day to protect the surrounding tissue. Sitz baths are used to cleanse the area. The patient is asked to notify the practitioner if she experiences increased vulvar swelling, malodorous drainage, erythema, bleeding from the procedure site, pain not resolved with NSAIDs, or a temperature of 100.5° F or higher. A follow-up appointment is scheduled for the patient 1 week after the initial TCA application. Depending on their size and shape, many warts fall off after a few applications of TCA.
Description of the simulation
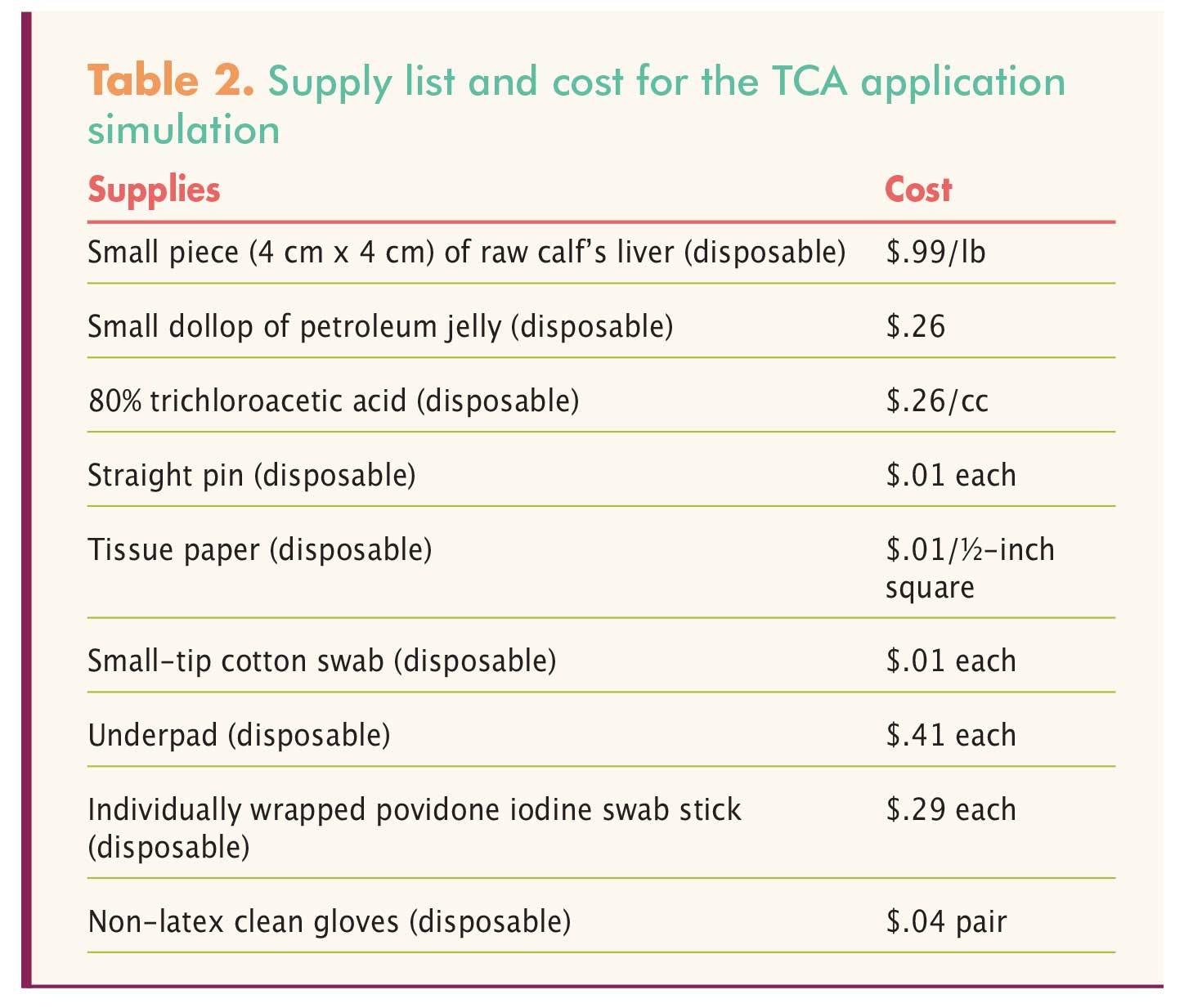
All of the supplies (Table 2) are easily obtained from a convenience store, grocery store, or online store. Supplies for this simulation are disposable and can be purchased at a cost of $2-$3. Liver is preferred; other meat sources will not blanch when TCA is applied. TCA is sold online and by medical supply companies.
{kind=link}
Step-by-step simulation assembly and video link
Wearing disposable gloves, the WHNP cuts a small piece (4 cm x 4 cm) of chilled, raw calf’s liver with the shiny sheath visible on top and places it on a disposable underpad. The shiny sheath of the liver will blanch with TCA application. The WHNP cuts a small piece of tissue paper into a ó inch x ó inch square and then molds it into a small ball with the thumb and index finger and secures it on the piece of liver with a straight pin to give the appearance of warts on the vulva (Photograph 6). Readers can access a video link for the TCA application simulation.*
Conclusion
Women’s health NPs need to know how to safely and accurately perform vulvar procedures, including a vulvar biopsy and condylomata acuminata treatment with TCA. The busy clinic setting does not provide novice WHNPs or WHNP students with an environment conducive to master newly learned procedures. Simulation learning can provide educational and clinical benefits to enhance practice.3 In a controlled, simulated envi ronment, learners can focus on achieving accuracy, confidence, and competence when performing vulvar procedures.3, 8
Aimee Chism Holland is Assistant Professor at the University of Alabama at Birmingham School of Nursing. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
Acknowledgment
The author heartily thanks Mr. James Clark, Instructional Design Specialist at the UAB School of Nursing, for recording these procedures for her.
References
1. Nakajima AK, Posner GD. Human Simulation for Women’s Health. New York, NY: Springer Publishing Company; 2012.
2. National League of Nursing Board of Governors. A Vision for Teaching with Simulation. April 20, 2015.
3. McGaghie WC, Issenberg SB, Cohen MR, et al. Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Acad Med. 2011;86(6):706-711.
4. Cooper S, Cant R, Porter J, et al. Simulation based learning in midwifery education: a systematic review. Women Birth. 2012;25(2):64-78.
5. Committee on Gynecologic Practice of American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 509: Management of vulvar intraepithelial neoplasia. Obstet Gynecol. 2011;118(5):1192 1194.
6. Sulik SM, Heath CB. Primary Care Procedures In Women’s Health. New York, NY: Springer Publishing Company; 2010.
7. CDC. Sexually transmitted diseases treatment guidelines. MMWR. Morbid Mortal Wkly Rep. 2015;64(3):84-90.
8. Nitschmann C, Bartz D, Johnson NR. Gynecologic simulation training increases medical student confidence and interest in women’s health. Teach Learn Med. 2014;26(2):160-163.
*These videos are the intellectual property of the University of Alabama at Birmingham and cannot be shared without request of a license (to do so, please contact the author at aimeeholland@uab.edu). However, NPWH members are encouraged to share the article itself, which contains links to the videos, with their colleagues.