
Editor’s Note: This article originally appeared in American Nurse Today, January 2018.
Acute care vs. chronic care is the key.
By Caroline Lloyd Doherty, AGACNP-BC; Patricia Pawlow, ACNP-BC; and Deborah Becker, PhD, ACNP-BC, CHSE, FAAN
As a current or future advanced practice nurse (APRN), you must understand the Consensus Model and its career implications to practice. The model was developed in 2008 by the APRN Consensus Work Group and the National Council of State Boards of Nursing APRN Advisory Committee. It was endorsed by more than 40 nursing organizations, including the American Association of Colleges of Nursing, National Organization of Nurse Practitioner Faculties, American Association of Nurse Anesthetists, American College of Nurse-Midwives, and the American Association of Nurse Practitioners.
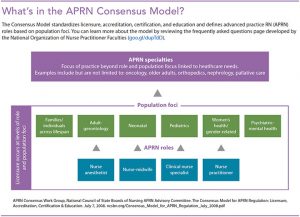
The Consensus Model addresses inconsistent standards in APRN education, regulation, and practice, which limited APRN mobility from one state to another. Through standardization of licensure, accreditation, certification, and education, the Consensus Model aims to improve access to APRN care. The model focuses on the four APRN roles: certified RN anesthetist (CRNA), certified nurse-midwife (CNM), clinical nurse specialist (CNS), and nurse practitioner (NP). It further specifies six population foci for APRN practice. (See What’s in the APRN Consensus Model?) Licensure and scope of practice are defined at the level of role and population foci, with the adult gerontology and pediatric NP roles delineated as acute care and primary care based on competencies obtained through formal education.
In this article, we’ll focus on the effect the Consensus Model has on working NPs and prospective students.
Consensus Model implications and challenges
 Until the early 1990s, NP education programs focused only on primary care. As NPs began to work with acutely ill patients in areas such as surgery, acute care NP programs were developed. However, these programs were scarce, compelling nurses with an interest in acute care to enroll in primary care programs. With the adoption of the Consensus Model, NPs with primary care preparation must return for formal acute care education and obtain certification as a condition of state licensure and maintenance of ongoing employment in their acute care role. This requirement aligns their scope of practice with the patients, diseases, and treatments they manage. However, confusion remains among some nurses, employers, and educators.
Until the early 1990s, NP education programs focused only on primary care. As NPs began to work with acutely ill patients in areas such as surgery, acute care NP programs were developed. However, these programs were scarce, compelling nurses with an interest in acute care to enroll in primary care programs. With the adoption of the Consensus Model, NPs with primary care preparation must return for formal acute care education and obtain certification as a condition of state licensure and maintenance of ongoing employment in their acute care role. This requirement aligns their scope of practice with the patients, diseases, and treatments they manage. However, confusion remains among some nurses, employers, and educators.
Some prospective NP students report being counseled to make themselves more marketable by combining acute care nursing experience with family NP education. This strategy doesn’t take into consideration the regulations that define and expand scope of practice by formal education only. NPs with primary care across-the-lifespan education aren’t prepared to care for acutely ill patients.
The model also affects NPs who work in specialties such as endocrinology or palliative care, where they manage patients with both chronic and acute care needs. Remember, educational requirements are determined by patient acuity, not the healthcare setting. However, interpretation of the model in these situations is inconsistent and may have job implications. One solution is dual certification.
Employers also struggle with interpretation of the Consensus Model, mistakenly hiring NPs prepared in primary care for hospitalist or other acute care positions. However, the only way for NPs to be properly prepared to manage acutely ill patients is to obtain formal education through completion of a dual master’s (primary and acute care–focused) or post-master’s program. Continuing education, fellowships, and on-the-job training aren’t sufficient.
Some hospital systems require NPs to return to school to obtain a post-master’s degree to meet Consensus Model requirements and as a condition of maintaining employment. The implications for NPs include time and expense; many post-master’s programs require up to seven courses and over 600 clinical hours. To facilitate the process for experienced NPs committed to aligning their practice with the Consensus Model, some universities have developed condensed programs. However, to ensure access and to support working NPs, schools must develop additional streamlined programs.
Some of these challenges may be why the Consensus Model, which had an implementation goal of 2015, has not yet been adopted by all U.S. states and territories. However, because many states, employers, and hospital systems have adopted the model, prospective APRNs must carefully choose a graduate program.
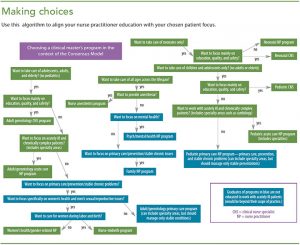
Choosing a program
To reduce the number of future NPs experiencing issues with their education and certification aligning with their scope of practice, we’ve developed an algorithm that illustrates a recommended process for choosing an APRN program. (See Making choices.) The first decision in the algorithm lets you determine the patient age range you’d like to manage. Next, you choose whether you want to be a CRNA, CNM, CNS, or NP. If you choose the NP route, you then decide whether you want to focus on acute care or chronic and preventive care.
Setting the standard
The Consensus Model has succeeded in setting standards for APRN preparation and practice. However, current challenges require communication among educators, employers, certifying bodies, and state boards of nursing about the model’s implementation to ensure its goal of increasing access to APRN practice is achieved.
The authors teach at the University of Pennsylvania School of Nursing in Philadelphia. Caroline Lloyd Doherty is teaching faculty for the adult gerontology acute care nurse practitioner program (AGACNP). Patricia Pawlow is the associate program director, and Deborah Becker is director of the AGACNP and adult gerontology clinical nurse specialist programs.
Selected references
APRN Consensus Work Group, National Council of State Boards of Nursing APRN Advisory Committee. Consensus Model for APRN Regulation: Licensure, Accreditation, Certification & Education. July 7, 2008.
National Organization of Nurse Practitioner Faculties. APRN Consensus Model: Frequently Asked Questions. August 19, 2010.
National Organization of Nurse Practitioner Faculties. Statement on Acute Care and Primary Care Certified Nurse Practitioner Practice 2012. June 2012.
Stanley JM. Impact of new regulatory standards on advanced practice registered nursing: The APRN Consensus Model and LACE. Nurs Clin North Am. 2012;47(2):241-50.