
The Zika virus, a mosquito-borne flavivirus,1 is becoming a growing concern for U.S. women in their childbearing years. The dramatic increase in the number of cases of Zika virus infection (ZVI), as well as its correlation with neurologic deficits (e.g., microcephaly in newborns), has made it crucial for healthcare providers (HCPs) to know as much as possible about identifying, treating, and preventing ZVI. This article offers up-to-date information for HCPs caring for reproductive-aged women—particularly those who are considering pregnancy or who are already pregnant— about when to test for ZVI, whom to test, and how to best inform patients about ZVI transmission and prevention.
CDC guidance for caring for pregnant women2
All pregnant women in the U.S. and U.S. territories should be assessed for possible Zika virus exposure at each prenatal care visit. Pregnant women should not travel to an area with active Zika virus transmission. Pregnant women who must travel to one of these areas should strictly follow steps to prevent mosquito bites during the trip. In addition, to avoid contracting ZVI, pregnant women whose sex partner has traveled to or resides in an area with active Zika virus transmission should use condoms or other barrier methods or abstain from sex for the duration of the pregnancy.
Part of the concern about ZVI is the lack of signs and symptoms (S/S) in up to 80% of persons infected and the vague, mild, flulike symptoms in the remaining portion, which makes identifying the disease so difficult. When S/S of ZVI do occur, they typically include rash, low-grade fever, arthralgia, fatigue, headache, and conjunctivitis.1 The rash, which tends to be the most prominent sign, is usually pruritic and maculopapular. It begins proximally and spreads to the extremities, with spontaneous resolution in 1-4 days.1
Symptomatic pregnant women
Pregnant women who report S/S of ZVI should be tested for it (Figure). Testing recommendations are the same regardless of the circumstances of possible exposure; however, the type of testing recommended depends on the time of evaluation relative to symptom onset. Testing of serum and urine by real-time reverse transcriptase polymerase chain reaction (rRT-PCR) is advised for pregnant women who seek care less than 2 weeks after symptom onset. This recommendation extends the previous recommendation for testing of serum from less than 1 week after symptom onset to less than 2 weeks. A positive rRT-PCR result confirms the diagnosis of recent maternal ZVI. Women with a negative rRT-PCR result should undergo both Zika virus IgM and dengue virus IgM antibody testing. If either antibody test yields positive or equivocal results, a plaque reduction neutralization test (PRNT) should be performed on the same IgM-tested sample or a subsequently collected sample to rule out false-positive results.
Pregnant women who seek care 2-12 weeks after symptom onset should first undergo Zika virus and dengue virus IgM antibody testing (see the Figure). If the Zika virus IgM antibody testing yields positive or equivocal results, reflex rRT-PCR testing should be automatically performed on the same serum sample to determine whether Zika virus RNA is present. A positive rRT-PCR result confirms the diagnosis of recent maternal ZVI. If the rRT-PCR result is negative, a positive or equivocal Zika virus IgM antibody test result should be followed by PRNT. Positive or equivocal dengue IgM antibody test results with a negative Zika virus IgM antibody test result should also be confirmed by PRNT.
Asymptomatic pregnant women
Testing recommendations for asymptomatic pregnant women with possible Zika virus exposure differ based on the circumstances of possible exposure (i.e., ongoing vs. limited exposure) and the elapsed interval since the last possible Zika virus exposure (see the Figure). Asymptomatic pregnant women living in areas without active Zika virus transmission who are evaluated less than 2 weeks after possible Zika virus exposure should be offered serum and urine rRT-PCR testing (see the Figure). A positive rRT-PCR result confirms the diagnosis of recent maternal ZVI. However, because viral RNA in serum and urine declines over time and depends on multiple factors, asymptomatic pregnant women with a negative rRT-PCR result require additional testing to exclude infection. These women should return 2-12 weeks after possible Zika virus exposure for Zika virus IgM antibody testing. A positive or equivocal IgM antibody test result should be confirmed by PRNT.
Asymptomatic pregnant women living in an area without active Zika virus transmission, and who seek care 2-12 weeks after possible Zika virus exposure, should be offered Zika virus IgM antibody testing (see the Figure). If the Zika virus IgM antibody test yields positive or equivocal results, reflex rRT-PCR testing should be performed on the same sample. If the rRTPCR result is negative, PRNT should be performed.
As recommended in previous guidance, IgM antibody testing is recommended as part of routine obstetric care during the first and second trimesters for asymptomatic pregnant women who have an ongoing risk for Zika virus exposure (i.e., residence in or frequent travel to an area with active Zika virus transmission) (see the Figure). Reflex rRT-PCR testing is recommended for women who have a positive or equivocal Zika virus IgM antibody test result because rRT-PCR testing provides the potential for a definitive diagnosis of ZVI. Negative rRT-PCR results after a positive or equivocal Zika virus IgM antibody test result should be followed by PRNT. The decision to implement testing of asymptomatic pregnant women with ongoing risk for Zika virus exposure should be made by local health officials based on information about levels of Zika virus transmission and laboratory capacity.
Symptomatic and asymptomatic pregnant women who seek care more than 12 weeks after symptom onset or possible Zika virus exposure
For these women, IgM antibody testing might be considered. If fetal abnormalities are present, rRT-PCR testing should also be performed on maternal serum and urine. However, a negative IgM antibody test or rRT PCR result more than 12 weeks after symptom onset or possible exposure does not rule out recent ZVI because IgM antibody and viral RNA levels decline over time. Given the limitations of testing beyond 12 weeks after symptom onset or possible exposure, serial fetal ultrasonography should be considered.
Management
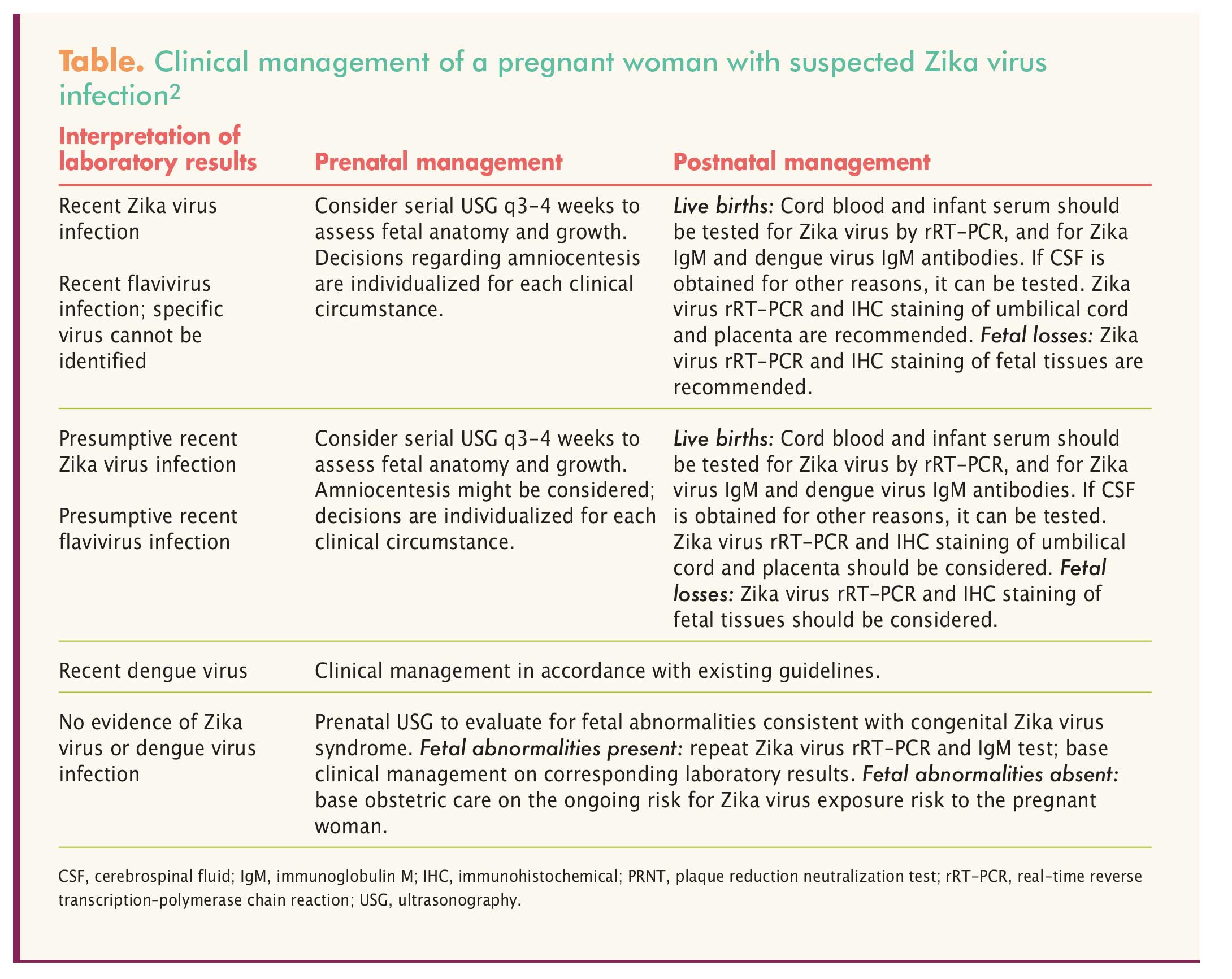
Management of confirmed ZVI is supportive, and includes rest, fluids, fever control, and analgesics.1 The Table provides recommendations for prenatal and postnatal management of pregnant women with laboratory evidence of confirmed or possible ZVI.2
{kind=link}
CDC guidance for HCPs caring for women of reproductive age3
Reproductive-aged women and their partners need counseling and education in accordance with their pregnancy intentions.
For couples who are not pregnant and are not planning to become pregnant in the near future
Healthcare providers should discuss strategies to prevent unintended pregnancy with these couples. When helping women choose a contraceptive method, its safety, effectiveness, availability, and acceptability should be considered. Women should be counseled to select the most effective method that they can use correctly and consistently. Long-acting reversible contraceptives, including subdermal implants and intrauterine devices, provide highly effective reversible birth control.
Couples in whom one partner has had possible Zika virus exposure will want to maximally reduce their risk for sexually transmitting Zika virus to the uninfected partner. They should use condoms consistently and correctly or abstain from sex for at least 6 months for men or 8 weeks for women after symptom onset (if symptomatic) or after the last possible Zika virus exposure (if asymptomatic). Some couples may choose to use condoms or abstain from sex for a shorter or longer period than recommended depending on their individual circumstances and risk tolerance.
For couples planning to conceive who do not live in areas with active Zika virus transmission
These couples should consider avoiding nonessential travel to areas with active Zika virus transmission. Women who have had possible Zika virus exposure through travel or sexual contact and do not have ongoing risks for exposure should wait at least 8 weeks from symptom onset (if symptomatic) or their last possible exposure (if asymptomatic) to attempt conception. Women who wait at least 8 weeks to conceive may have an increased likelihood that Zika virus no longer presents a risk for maternal–fetal transmission.
The CDC recommends that men with possible Zika virus exposure, regardless of symptom status, wait at least 6 months from symptom onset (if symptomatic) or their last possible exposure (if asymptomatic) before attempting conception with their partner. The recommendation to wait at least 6 months for asymptomatic men, as opposed to the previous recommendation to wait at least 8 weeks, is based on the range of time after symptom onset that Zika virus RNA has been detected in semen of symptomatic men and the absence of definitive data that the risk for sexual transmission differs between symptomatic and asymptomatic men. Zika virus has not been definitively cultured from semen more than 3 months after symptom onset. It is unknown whether detection of Zika virus RNA in semen indicates presence of infectious virus and the potential for transmission.
For couples who want to conceive, in which one or both partners live in areas with active Zika virus transmission
For these couples, any partner who experiences symptoms of ZVI should be tested for it. Men with results that indicate recent ZVI or unspecified flavivirus infection should wait at least 6 months from symptom onset to attempt conception with their partner; women with results that indicate recent ZVI or unspecified flavivirus infection should wait at least 8 weeks from symptom onset to attempt conception. Partners who have had symptoms of ZVI with negative Zika virus test results should talk with their HCP about timing of conception in the setting of ongoing risk for possible exposure.
Couples living in an area with active Zika virus transmission should be counseled on the possible risk for ZVI during the periconception period. The CDC has developed tools to assist HCPs with preconception counseling. HCPs should provide counseling about the potential consequences to the fetus associated with ZVI during pregnancy, such as microcephaly and other serious brain abnormalities. Women should discuss their reproductive life plans with their HCP, in the context of potential and ongoing Zika virus exposure. HCPs should review factors that might influence pregnancy timing (e.g., unknown duration of Zika virus outbreak, fertility, age, reproductive history, health history, personal values and preferences). For couples who choose to conceive, HCPs should emphasize the use of mosquito bite prevention strategies while attempting pregnancy and during pregnancy.
Conclusion
The Zika virus has been declared a public health emergency because of the ease of transmission, the relatively benign and asymptomatic viral infection it causes, and its correlation with major neurologic complications in newborns whose mothers contracted ZVI during pregnancy. A continued response from government agencies, local health officials, HCPs, and researchers remains underway to shed new light onto this growing concern. As this epidemic continues to unfold, it remains crucial to educate women of childbearing age and their partners about the inherent risks of the Zika virus and avoidance of infection.
Jessica L. Isnetto is a faculty member at Kaplan University in Orlando, Florida. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
1. Ploudre AR, Bloch EM. A literature review of Zika virus. Emerg Infect Dis. 2016;22(7):1185-1192.
2. CDC. Update: Interim Guidance for Health Care Providers Caring for Pregnant Women with Possible Zika Virus Exposure — United States, July 2016.
3. CDC. Update: Interim Guidance for Preconception Counseling and Prevention of Sexual Transmission of Zika Virus for Persons with Possible Zika Virus Exposure — United States, September 2016.